


For most Americans, regardless of their education or background, health insurance can be tricky to navigate. For Black, Indigenous, and other people of color, these barriers are not just inconveniences – they’re baked in inequities.

With the passage of a federal budget bill (also known as HR1 or the One Big Beautiful Bill Act), new federal policy changes are poised to make things even more challenging. In particular, new work reporting requirements and eligibility reviews for HUSKY D enrollees beginning in 2027 are not simply a tweak to Medicaid – they introduce sweeping new administrative burdens that will push eligible people out of coverage.
Such policies reinforce the notion of the “deserving poor” and rely on inaccurate assumptions that ignore the reality that the vast majority of Medicaid enrollees already work, are students or caregivers, or live with a disability that can limit their access to a steady income. The real impact of increased red tape is not accountability but rather increased inequity.
Further, working and proving that one is working are two separate processes. Connecticut’s HUSKY program projects that over 100,000 enrollees will lose coverage due to new work reporting requirements alone even though estimates suggest that the majority of Medicaid enrollees are already working or exempt. Why? These policies make enrollees’ access to health care contingent on their ability to jump through hoops, understand complex policy details, and navigate complicated online systems.
An analysis of work reporting requirements prepared for Congress found that prior efforts to impose such requirements on Medicaid enrollees have had very little impact on employment rates but have caused significant coverage losses. In other words, the real impact of more red tape is not accountability, but rather loss of coverage for working people, which leads to delayed care, economic losses for health care providers, and preventable illness and death.
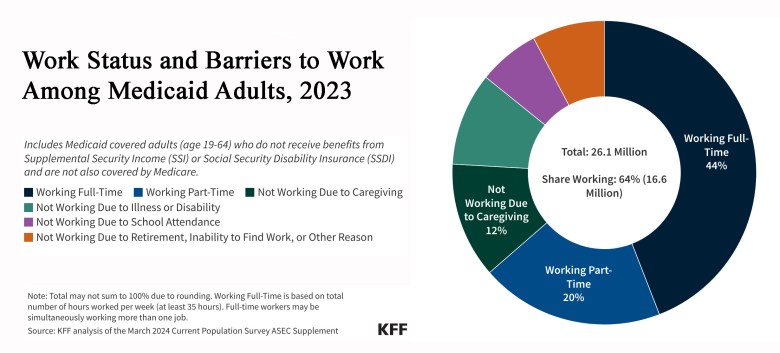
The driving force behind these new work reporting requirements is the racist stereotype that Medicaid enrollees (who are disproportionately, though not majority, Black and Latino) are “lazy” and aren’t doing enough to earn their benefits. Contrary to this racist myth, 92% of working-age adults on Medicaid are either working, in school, providing care for a child or relative, or are unable to work due to illness or disability.
Work reporting requirements do not promote employment. Instead, they force low-income people, who are more likely to experience unpredictable work hours and unstable job security to prove their “worthiness.” In addition to outright coverage losses, many individuals will be plunged into a cycle of “churn” in which they disenroll and reenroll within a short time frame, disrupting access to care and increasing the state’s administrative workload.
While the state is compelled to implement these racist and ineffective policies, we have many opportunities to mitigate their harm.
In addition to imposing punitive work requirements, HR1 includes provisions that harm immigrants. Under this law, starting in October, there will be no Medicaid and CHIP funding for refugees, asylees, and certain other noncitizens. Premium tax credits were eliminated for low-income immigrants who have lived in the U.S. for less than five years on January 1, 2026. The majority of U.S. immigrants are likely people of color, which means disenrollment will unfairly burden people of color. These provisions create an environment where accessing basic health care becomes more precarious for immigrant families. They will be forced to navigate paperwork to prove their immigration status and prevent them from accessing health care altogether, in fear of immigration enforcement. Further, due to fear and confusion, some eligible immigrants will also lose coverage, which will exacerbate racial inequities in health coverage.
We urge our state leaders to:
- Co-design processes and systems with enrollees, rather than developing such systems without input from the people who will be required to use them. This is crucial to the efficiency of processes for requesting exemptions and proving work status.
- Engage trusted community partners to conduct targeted outreach and provide support as work requirements are developed and implemented. Many Connecticut residents are already confused and concerned about their eligibility for HUSKY.
- Simplify the reporting and enrollment process within the bounds of existing guidance without waiting for federal regulations (which will almost certainly be released after decisions about these new systems have been made).
- Engage with enrollees and monitor enrollment/renewal data to track inequities in coverage loss and opportunities to improve inefficiencies in new systems.
- Invest in new coverage solutions for people who lose access to Medicaid or are priced out of Access Health due to HR1.
At its core, this law will create a system that punishes us all. When our neighbors don’t have access to health care, they struggle to work and care for their families. When some of us are left behind, we all lose. We lose the strength of a healthy workforce and the stability of families who can fully participate in their communities. We lose the economic contributions of healthy people and the stability of our health systems (which rely on funding from HUSKY and other health coverage).
Increasing administrative burdens, imposing work requirements, creating new fees, and stripping health care coverage away from immigrants will disproportionately impact Black and brown communities the most and widen the health and racial inequities that already exist.
But Connecticut can mitigate the damage by taking the steps outlined above and by investing in coverage solutions for those who will inevitably be unable to stay enrolled in HUSKY programs. Our leaders did not create this crisis BUT they are both obligated AND able to address it.
Because make no mistake: HR1 isn’t just bad policy — it’s death by paperwork, and Black and brown communities will pay the highest price.
Ayesha R. Clarke serves as the Executive Director of Health Equity Solutions and as the Co-Chair of the Advisory Body of the Commission on Racial Equity in Public Health.
