



Officials and medical professionals predict that Fairfield and New Haven county will experience the COVID-19 peak outbreak by the end of April; Hartford County will follow in May. Our collective medical response to the unprecedented and catastrophic pandemic accentuated overall societal weaknesses, particularly with regard to inequality and marginalization.

While media outlets have reported on how the pandemic tragically leaves certain groups behind, and whereas much has been made with regard to presidential declarations concerning a “Chinese virus,” very little attention has been paid to the needs of one under-represented group: the state’s sizeable Southeast Asian-American population.
Among the state’s minority groups, Southeast Asian-Americans are significant but often invisible. Such invisibility is in part due to demographic reporting: about half of the more than 200,000 Asian-Americans in Connecticut claim India or China (PRC) as their national origin or heritage. These Asian-Americans frequently possesses technical skills, speak English, and earn higher than average incomes. Together, Southeast Asian- Americans —which include Burmese, Cambodian, Filipino, Hmong, Indonesian, Karen, Laotian, Malaysian, Thai, and Vietnamese Americans — constitute 25% of the larger Asian-American racial category in the state. Despite such ethnic diversity, Southeast Asian-Americans are, due to racial assumptions which assume that all Asian-Americans are “the same,” are frequently absent from state policy and ignored in Connecticut politics.
This wholesale characterization of Asian-Americans prohibits serious discussions involving specific issues faced by Southeast Asian-Americans, particularly with regard to income inequality, health disparity, and language. Because many Vietnamese, Laotian, Hmong, and Cambodians came to the United States as refugees of the Vietnam War, these populations must contend with the historical legacy of torture and involuntary displacement.
Such experiences with human rights violation are often forgotten due to the mainstream understanding that Asian-Americans are “model minorities.” As model minorities, Asian-Americans are understood as a privileged, homogenous group that has achieved aspirational socioeconomic success and high academic achievement. However, as is the case with all populations, not all Asian-American experiences are the same. Nor are all Asian- Americans “model minorities,” a point made abundantly clear over the course of this pandemic.
The rise in anti-Asian racism has followed the COVID-19 pandemic and has led to hate crimes, attacks, harassment, vandalism and threats to not just Chinese Americans, but Asian-Americans of many backgrounds. More than a 1,000 incidents have been reported in February across the country and analysis of incident reports shows that Asian-American women are more likely to be targeted.
Racist language, scapegoating, and conspiracy theories continue to be a part of the Trump administration and GOP response to the COVID-19 pandemic, fueling racial violence and hatred of Asians as well as a number of other groups including Jews and LGBTQ people. These distortions and dangerous speech acts have health consequences.
Racism makes the pandemic worse in at least three ways. First it deters scientific understanding from the epidemiological reality to the social construct. Second, racial blame in pandemics leads to violence and retribution against innocent people, and also discourages the targeted from seeking care for fear of attacks. Third, assigning racial blame in a pandemic creates a false sense of security that the disease only afflicts other people.
In order to assist health care providers and other service operators in the state, this article provides some useful information to increase access to medical interpreters and disseminate knowledge about the Southeast Asian- American population. In order to visually represent the location and size of these populations, interactive maps have been included to show the approximate distribution of the Asian American population in the state.
I made this map to display the extent of the Southeast Asian American population in the state and this other map shows the total Asian American population as counted in 2017.
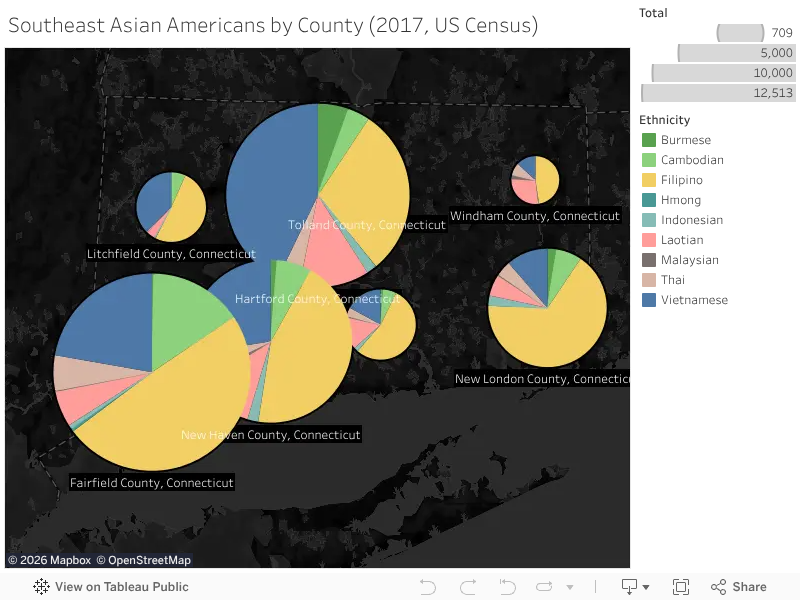
Fairfield, New Haven, and Hartford Counties have the highest concentrations of Southeast Asian-Americans in the state. Filipinos, Vietnamese, Cambodians, and Laotians form the largest groups of Southeast Asian- Americans, but include others.
Due to the health disparities already faced by these groups they are more vulnerable to serious consequences of a COVID-19 infection. Recent research from around the country has verified what many feared, that the COVID-19 pandemic will have disparate impacts along existing lines of inequality. The effects are uneven because the legacies of racial oppression and continuous discrimination have stripped black and brown people of resources, prevented their upward mobility, and denied them access to appropriate care.
For example, Essence reports that Black people account for 40% of COVID-19 deaths in Michigan but only make up 14% of the state’s population. Likewise, the Pew Research Center has shown that Latinos are 10-20% more likely than all other Americans to experience a pay cut or job loss due to COVID-19 shutdowns. Southeast Asian- Americans are a smaller population but share similar conditions as other larger non-white racial groups. An additional dimension of vulnerability is that almost 10% of Asian-Americans in Connecticut are employed in healthcare and medicine, while only representing 5% of the state’s population. The majority of these Asian- Americans are Filipino nurses and are exposed to far greater risks of infection as they work with patients during this surge.
This census data identifies populations with specific language needs to address prescriptive actions such as social distancing as well as the need for interpreters to receive medical care. The Asian & Pacific Islander Health Forum has constructed a list of basic COVID-19 medical information in thirty languages.
Mary Scully, of Khmer Health Advocates (KHA) in West Hartford, estimates that “a minimum of 65% of Southeast Asian-Americans would require a medical interpreter on a good day, assuming the patient is not under stress.” Rachel Legg of the KHA notes that, “approximately 65% of Cambodians (over 40) do not speak sufficient English to understand medical instructions,” adding that, “a similar number are illiterate in English and Khmer.” These language skills are needed because Legg underscores the fact that “Cambodians are among the highest risk people in Connecticut due to extremely high rates of Post-Traumatic Stress Disorder (PTSD) (65%), diabetes and pre-diabetes (49%), as well as, hypertension (45%).”
Medical professionals know that stress and resulting high cortisol levels aggravates existing conditions and increases the likelihood of health complications. Advocates of Southeast Asian-Americans in the state are concerned that economic hardship (including layoffs and closed businesses), alienation from social distancing, and the increase in racial violence are pushing this vulnerable population to a dangerous threshold.
The KHA’s closest connections are with the Laotian and Vietnamese communities in Connecticut. The main languages spoken by the Cambodian, Laotian and Vietnamese populations are Khmer, Vietnamese, Lao. Currently, if individuals seek healthcare at locations that accept federal funding, then healthcare providers are required to furnish language services free of charge. Legg notes that “the interpretation is not always of optimum quality and often over the phone or Skype, but it will be provided.”
In the context of scarcity during the surge of COVID-19 infections and hospitalizations, the medical interpreters will also be in high demand. “Right now the Southeast Asian-American communities do not have a lot of resources to provide general interpretation but [organizations] can guide people in locating and connecting with services.” Legg said. Rising unemployment in the state is disturbing the KHA’s connection with their patients during this difficult time. This is why it is all the more important for doctors, clinicians, and medical professionals to have resources at the ready.
Khmer Health Advocates (community-based organization for the Cambodian community)
860.561.3345 (KHA office phone transfers to cell phones.)
Vietnamese organization/CMAA (CT mutual assistance association)
860.236.6452 (Work)
860.380.7067 (Cell)
Lao Association
860.523.834O (Work)
860.573.4286 (Cell)
2020 Census
The current federal census could be an excellent tool to maintain accurate information about the Southeast Asian- American population. However, there are some challenges for achieving a robust count of this population. KHA notes that language barriers, PTSD, multi-family households, and mixed-immigration status families will complicate counts of Southeast Asian-Americans.
More than the social and mental health features of the population, politics appear to be the main obstacle to strong participation in the census. Legg of the KHA notes that “fears of deportations, even from naturalized citizens, leads to fear of the government and [people] will be less likely to participate.” She remarked that her clients’ referenced President Trump’s anti-immigrant, anti-refugee rhetoric and policies as the source of this fear.
Despite the need for collecting and maintaining ethnically disaggregated data, some Asian-Americans in the state have moved to prevent authorities from doing so for schools. Critics of maintaining disaggregated data stem from unfounded concerns that ethnic identifiers could be used to limit access to higher education.
Supporters of the Connecticut bill to prohibit the collection of student data claim that ethnic identifiers always lead to discrimination and targeting. It does not follow logically that because past discrimination has identified specific groups through data, that ending data collection will prevent future discrimination. Eliminating disaggregated data will simply mean that discrimination will be harder to identify. Data is the bedrock of effective public policy. The COVID-19 pandemic shows how vital maintaining data about our communities is to sustaining the health and well-being of everyone.
Despite these concerns there is hope that the census will “capture the true poverty that many of our community members live in and how hard they work,” Legg said. She went on to highlight, “Manufacturing jobs sound a lot less serious on paper but can be very taxing work and community members are often underpaid and [are] getting older.”
Advocates remain concerned, however. Since the census does not collect health data, this remains an important yet unanswered question. Legg reiterates, “Health data has the biggest impact for the SEA community both in broadcasting the unique needs of the community and also communicating that the community has unique needs so they deserve attention from our government and healthcare system.” A unique dimension is the impact of trauma from war, confinement, torture, and displacement. Legg notes, “It is layered into every part of their life and the census will not capture how serious the community and personal trauma is, and how debilitating it can be.”
Jason Oliver Chang is an Associate Professor of History and Asian/Asian American Studies at the University of Connecticut. He is also Director of the Asian and Asian-American Studies Institute.
Acknowledgements: This article was written with the help of Cora Chang, Angela Rola, Cathy Schlund-Vials, Megan Berthold, Rachel Legg and Mary Scully. Data is derived from U.S. Census figures, 2017.
