


The U.S. public health system has been starved for decades and lacks the resources to confront the worst health crisis in a century.
Marshaled against a virus that has sickened at least 2.6 million in the U.S., killed more than 129,000 people and cost tens of millions of jobs and $3 trillion in federal rescue money, state and local government health workers on the ground are sometimes paid so little that they qualify for public aid.
They track the coronavirus on paper records shared via fax. Working seven-day weeks for months on end, they fear pay freezes, public backlash and even losing their jobs.
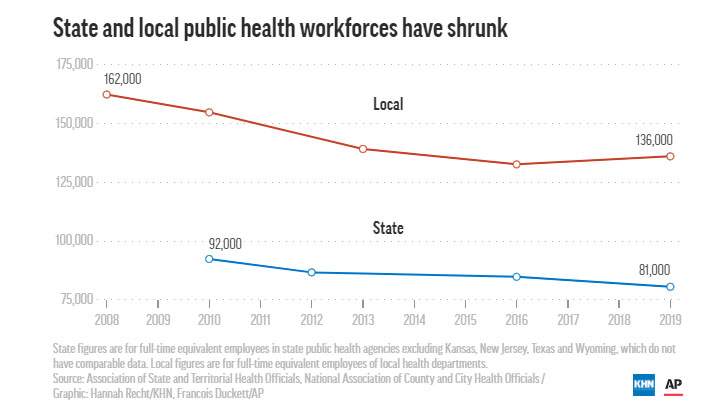
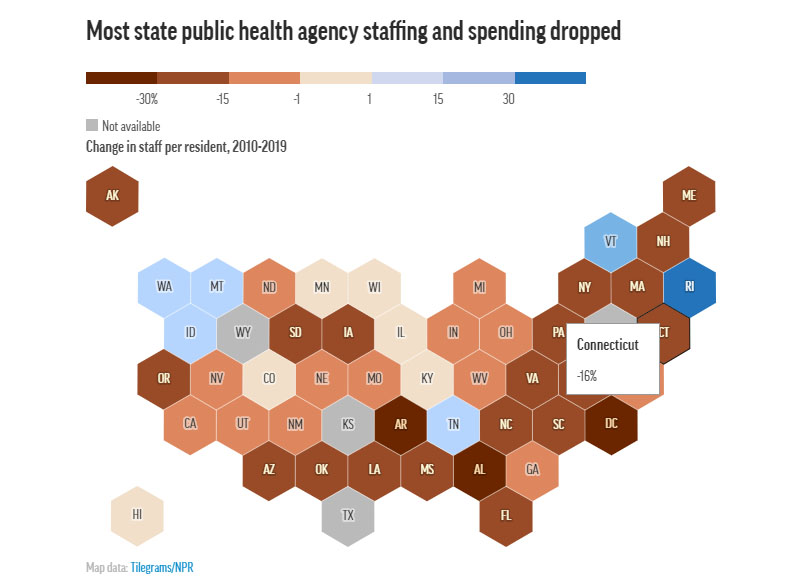
Since 2010, spending for state public health departments has dropped by 16% per capita and spending for local health departments has fallen by 18%, according to a KHN and Associated Press analysis of government spending on public health. At least 38,000 state and local public health jobs have disappeared since the 2008 recession, leaving a skeletal workforce for what was once viewed as one of the world’s top public health systems.
KHN and AP interviewed more than 150 public health workers, policymakers and experts, analyzed spending records from hundreds of state and local health departments, and surveyed statehouses. On every level, the investigation found, the system is underfunded and under threat, unable to protect the nation’s health.
Dr. Robert Redfield, the director of the Centers for Disease Control and Prevention, said in an interview in April that his “biggest regret” was “that our nation failed over decades to effectively invest in public health.”
So when this outbreak arrived — and when, according to public health experts, the federal government bungled its response — hollowed-out state and local health departments were ill-equipped to step into the breach.
Over time, their work had received so little support that they found themselves without direction, disrespected, ignored, even vilified. The desperate struggle against COVID-19 became increasingly politicized and grew more difficult.
States, cities and counties in dire straits have begun laying off and furloughing members of already limited staffs, and even more devastation looms, as states reopen and cases surge. Historically, even when money pours in following crises such as Zika and H1N1, it disappears after the emergency subsides. Officials fear the same thing is happening now.
“We don’t say to the fire department, ‘Oh, I’m sorry. There were no fires last year, so we’re going to take 30% of your budget away.’ That would be crazy, right?” said Dr. Gianfranco Pezzino, the health officer in Shawnee County, Kansas. “But we do that with public health, day in and day out.”
Ohio’s Toledo-Lucas County Health Department spent $17 million, or $40 per person, in 2017.
Jennifer Gottschalk, 42, works for the county as an environmental health supervisor. When the coronavirus struck, the county’s department was so short-staffed that her duties included overseeing campground and pool inspections, rodent control and sewage programs, while also supervising outbreak preparedness for a community of more than 425,000 people.
When Gottschalk and five colleagues fell ill with COVID-19, she found herself fielding calls about a COVID-19 case from her hospital bed, then working through her home isolation. She stopped only when her coughing was too severe to talk on calls.
“You have to do what you have to do to get the job done,” Gottschalk said.
Now, after months of working with hardly a day off, she said the job is wearing on her. So many lab reports on coronavirus cases came in, the office fax machine broke. She faces a backlash from the community over coronavirus restrictions and there are countless angry phone calls.
Things could get worse; possible county budget cuts loom.
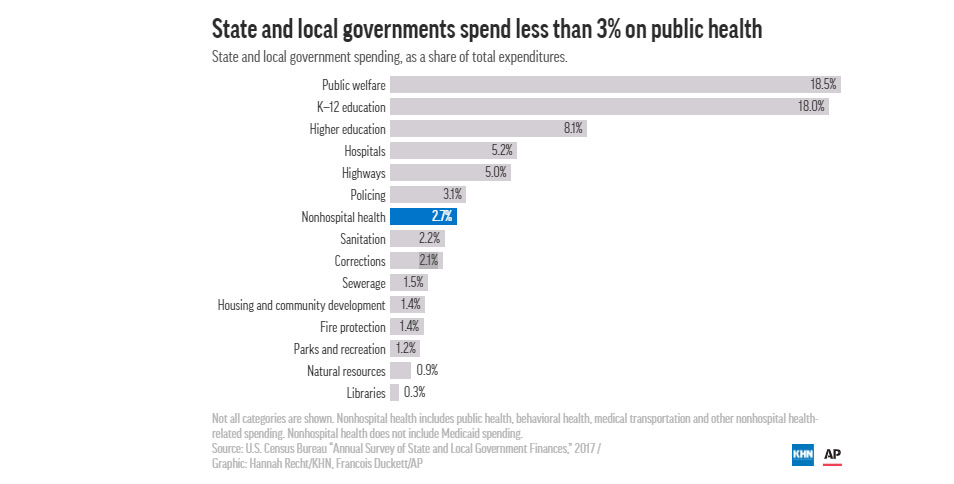
But Toledo-Lucas is no outlier. Public health ranks low on the nation’s financial priority list. Nearly two-thirds of Americans live in counties that spend more than twice as much on policing as they spend on non-hospital health care, which includes public health.
More than three-quarters of Americans live in states that spend less than $100 per person annually on public health. Spending ranges from $32 in Louisiana to $263 in Delaware, according to data provided to KHN and AP by the State Health Expenditure Dataset project.
That money represents less than 1.5% of most states’ total spending, with half of it passed down to local health departments.
The share of spending devoted to public health belies its multidimensional role. Agencies are legally bound to provide a broad range of services, from vaccinations and restaurant inspections to protection against infectious disease. Distinct from the medical care system geared toward individuals, the public health system focuses on the health of communities at large.
“Public health loves to say: When we do our job, nothing happens. But that’s not really a great badge,” said Scott Becker, chief executive officer of the Association of Public Health Laboratories. “We test 97% of America’s babies for metabolic or other disorders. We do the water testing. You like to swim in the lake and you don’t like poop in there? Think of us.”
But the public doesn’t see the disasters they thwart. And it’s easy to neglect the invisible.
A history of deprivation
The local health department was a well-known place in the 1950s and 1960s, when Harris Pastides, president emeritus of the University of South Carolina, was growing up in New York City.
“My mom took me for my vaccines. We would get our injections there for free. We would get our polio sugar cubes there for free,” said Pastides, an epidemiologist. “In those days, the health departments had a highly visible role in disease prevention.”
The United States’ decentralized public health system, which matches federal funding and expertise with local funding, knowledge and delivery, was long the envy of the world, said Saad Omer, director of the Yale Institute for Global Health.
“A lot of what we’re seeing right now could be traced back to the chronic funding shortages,” Omer said. “The way we starve our public health system, the way we have tried to do public health outcomes on the cheap in this country.”
In Scott County, Indiana, when preparedness coordinator Patti Hall began working at the health department 34 years ago, it ran a children’s clinic and a home health agency with several nurses and aides. But over time, the children’s clinic lost funding and closed. Medicare changes paved the way for private services to replace the home health agency. Department staff dwindled in the 1990s and early 2000s. The county was severely outgunned when rampant opioid use and needle sharing sparked an outbreak of HIV in 2015.
Besides just five full-time and one part-time county public health positions, there was only one doctor in the outbreak’s epicenter of Austin. Indiana’s then-Gov. Mike Pence, now leading the nation’s coronavirus response as vice president, waited 29 days after the outbreak was announced to sign an executive order allowing syringe exchanges. At the time, a state official said that only five people from agencies across Indiana were available to help with HIV testing in the county.
The HIV outbreak exploded into the worst ever to hit rural America, infecting more than 230 people.
At times, the federal government has promised to support local public health efforts, to help prevent similar calamities. But those promises were ephemeral.
Two large sources of money established after Sept. 11, 2001 — the Public Health Emergency Preparedness program and the Hospital Preparedness Program — were gradually chipped away.
The Affordable Care Act established the Prevention and Public Health Fund, which was supposed to reach $2 billion annually by 2015. The Obama administration and Congress raided it to pay for other priorities, including a payroll tax cut. The Trump administration is pushing to repeal the ACA, which would eliminate the fund, said Carolyn Mullen, senior vice president of government affairs and public relations at the Association of State and Territorial Health Officials.
Former Iowa Sen. Tom Harkin, a Democrat who championed the fund, said he was furious when the Obama White House took billions from it, breaking what he said was an agreement.
“I haven’t spoken to Barack Obama since,” Harkin said.

If the fund had remained untouched, an additional $12.4 billion would eventually have flowed to local and state health departments.
But local and state leaders also did not prioritize public health over the years.
In Florida, for example, 2% of state spending goes to public health. Spending by local health departments in the state fell 39%, from a high of $57 in inflation-adjusted dollars per person in the late 1990s to $35 per person last year.
In North Carolina, Wake County’s public health workforce dropped from 882 in 2007 to 614 a decade later, even as the population grew by 30%.
In Detroit, the health department had 700 employees in 2009, then was effectively disbanded during the city’s bankruptcy proceedings. It’s been built back up, but today still has only 200 workers for 670,000 residents.
Many departments rely heavily on disease-specific grant funding, creating unstable and temporary positions. The CDC’s core budget, some of which goes to state and local health departments, has essentially remained flat for a decade. Federal money currently accounts for 27% of local public health spending.
Years of such financial pressure increasingly pushed workers in this predominantly female workforce toward retirement or the private sector and kept potential new hires away.
More than a fifth of public health workers in local or regional departments outside big cities earned $35,000 or less a year in 2017, as did 9% in big-city departments, according to research by the Association of State and Territorial Health Officials and the de Beaumont Foundation.
Even before the pandemic, nearly half of public health workers planned to retire or leave their organizations for other reasons in the next five years. Poor pay topped the list of reasons.
Armed with a freshly minted bachelor’s degree, Julia Crittendon took a job two years ago as a disease intervention specialist with Kentucky’s state health department. She spent her days gathering detailed information about people’s sexual partners to fight the spread of HIV and syphilis. She tracked down phone numbers and drove hours to pick up reluctant clients.
The mother of three loved the work but made so little money that she qualified for Medicaid, the federal-state insurance program for America’s poorest. Seeing no opportunity to advance, she left.
“We’re like the redheaded stepchildren, the forgotten ones,” said Crittendon, 46.

Such low pay is endemic, with some employees qualifying for the nutrition program for new moms and babies that they administer. People with the training for many public health jobs, which can include a bachelor’s or master’s degree, can make much more money in the private health care sector, robbing the public departments of promising recruits.
Dr. Tom Frieden, a former CDC director, said the agency “intentionally underpaid people” in a training program that sent early-career professionals to state and local public health departments to build the workforce.
“If we paid them at the very lowest level at the federal scale,” he said in an interview, “they would have to take a 10-20% pay cut to continue on at the local health department.”
As low pay sapped the workforce, budget cuts sapped services.
In Alaska, the Division of Public Health’s spending dropped 9% from 2014 to 2018 and staffing fell by 82 positions in a decade to 426. Tim Struna, chief of public health nursing in Alaska, said declines in oil prices in the mid-2010s led the state to make cuts to public health nursing services. They eliminated well-child exams for children over 6, scaled back searches for the partners of people with certain sexually transmitted infections and limited reproductive health services to people 29 and younger.
Living through an endless stream of such cuts and their aftermath, those workers on the ground grew increasingly worried about mustering the “surge capacity” to expand beyond their daily responsibilities to handle inevitable emergencies.
When the fiercest of enemies showed up in the U.S. this year, the depleted public health army struggled to hold it back.
A decimated surge capacity
As the public health director for the Kentucky River District Health Department in rural Appalachia, Scott Lockard is battling the pandemic with 3G cell service, paper records and one-third of the employees the department had 20 years ago.
He redeployed his nurse administrator to work round-the-clock on contact tracing, alongside the department’s school nurse and the tuberculosis and breastfeeding coordinator. His home health nurse, who typically visits older patients, now works on preparedness plans. But residents aren’t making it easy on them.
“They’re not wearing masks, and they’re throwing social distancing to the wind,” Lockard said in mid-June, as cases surged. “We’re paying for it.”
Even with more staff since the HIV outbreak, Indiana’s Scott County Health Department employees worked evenings, weekends and holidays to deal with the pandemic, including outbreaks at a food packing company and a label manufacturer. Indiana spends $37 a person on public health.
“When you get home, the phone never stops, the emails and texts never stop,” said Hall, the preparedness coordinator.
All the while, she and her colleagues worry about keeping HIV under control and preventing drug overdoses from rising. Other health problems don’t just disappear because there is a pandemic.
“We’ve been used to being able to ‘MacGyver’ everything on a normal day, and this is not a normal day,” said Amanda Mehl, the public health administrator for Boone County, Illinois, citing a TV show.
Pezzino, whose department in Kansas serves Topeka and Shawnee County, said he had been trying to hire an epidemiologist, who would study, track and analyze data on health issues, since he came to the department 14 years ago. Finally, less than three years ago, they hired one. She just left, and he thinks it will be nearly impossible to find another.
While epidemiologists are nearly universal in departments serving large populations, hardly any departments serving smaller populations have one. Only 28% of local health departments have an epidemiologist or statistician.
Strapped departments are now forced to spend money on contact tracers, masks and gloves to keep their workers safe and to do basic outreach.
Melanie Hutton, administrator for the Cooper County Public Health Center in rural Missouri, pointed out the local ambulance department got $18,000, and the fire and police departments got masks to fight COVID-19.
“For us, not a nickel, not a face mask,” she said. “We got [5] gallons of homemade hand sanitizer made by the prisoners.”
Public health workers are leaving in droves. At least 34 state and local public health leaders have announced their resignations, retired or been fired in 17 states since April, a KHN-AP review found. Others face threats and armed demonstrators.
Ohio’s Gottschalk said the backlash has been overwhelming.
“Being yelled at by residents for almost two hours straight last week on regulations I cannot control left me feeling completely burned out,” she said in mid-June.
Many are putting their health at risk. In Prince George’s County, Maryland, public health worker Chantee Mack died after, family and co-workers believe, she and several colleagues contracted the disease in the office.
A difficult road ahead
Pence, in an op-ed in The Wall Street Journal on June 16, said the public health system was “far stronger” than it was when the coronavirus hit.
It’s true that the federal government this year has allocated billions for public health in response to the pandemic, according to the Association of State and Territorial Health Officials. That includes more than $13 billion to state and local health departments, for activities including contact tracing, infection control and technology upgrades.
A KHN-AP review found that some state and local governments are also pledging more money for public health. Alabama’s budget for next year, for example, includes $35 million more for public health than it did this year.
But overall, spending is about to be slashed again as the boom-bust cycle continues.
In most states, the new budget year begins July 1, and furloughs, layoffs and pay freezes have already begun in some places. Tax revenues evaporated during lockdowns, all but ensuring there will be more. At least 14 states have already cut health department budgets or positions or were actively considering such cuts in June, according to a KHN-AP review.
Since the pandemic began, Michigan temporarily cut most of its state health workers’ hours by one-fifth. Pennsylvania required more than 65 of its 1,200 public health workers to go on temporary leave, and others lost their jobs. Knox County, Tennessee, furloughed 26 out of 260 workers for eight weeks.
Frieden, formerly of the CDC, said it’s “stunning” that the U.S. is furloughing public health workers amid a pandemic. The country should demand the resources for public health, he said, just the way it does for the military.
“This is about protecting Americans,” Frieden said.
Cincinnati temporarily furloughed approximately 170 health department employees.
Robert Brown, chair of Cincinnati’s Primary Care Board, questions why police officers and firefighters didn’t face similar furloughs at the time or why residents were willing to pay hundreds of millions in taxes over decades for the Bengals’ football stadium.
“How about investing in something that’s going to save some lives?” he asked.
In 2018, Boston spent five times as much on its police department as its public health department. The city recently pledged to transfer $3 million from its approximately $60 million police overtime budget to its public health commission.
Looking ahead, more cuts are coming. Possible budget shortfalls in Brazos County, Texas, may force the health department to limit its mosquito-surveillance program and eliminate up to one-fifth of its staff and one-quarter of immunization clinics.
Months into the pandemic response, health departments are still trying to ramp up to fight COVID-19. Cases are surging in states including Texas, Arizona and Florida.
Meanwhile, childhood vaccinations began plunging in the second half of March, according to a CDC study analyzing supply orders. Officials worry whether they will be able to get kids back up to date in the coming months. In Detroit, the childhood vaccination rate dipped below 40%, as clinics shuttered and people stayed home, creating the potential for a different outbreak.
Cutting or eliminating non-COVID activities is dangerous, said E. Oscar Alleyne, chief of programs and services at the National Association of County and City Health Officials. Cuts to programs such as diabetes control and senior nutrition make already vulnerable communities even more vulnerable, which makes them more likely to suffer serious complications from COVID. Everything is connected, he said.
It could be a year before there’s a widely available vaccine. Meanwhile, other illnesses, including mental health problems, are smoldering.
The people who spend their lives working in public health say the temporary coronavirus funds won’t fix the eroded foundation entrusted with protecting the nation’s health as thousands continue to die.
Contributing to this report were: Associated Press writers Mike Stobbe in New York; Mike Householder in Toledo, Ohio; Lindsay Whitehurst in Salt Lake City, Utah; Brian Witte in Annapolis, Maryland; Jim Anderson in Denver; Sam Metz in Carson City, Nevada; Summer Ballentine in Jefferson City, Missouri; Alan Suderman in Richmond, Virginia; Sean Murphy in Oklahoma City, Oklahoma; Mike Catalini in Trenton, New Jersey; David Eggert in Lansing, Michigan; Andrew DeMillo in Little Rock, Arkansas; Jeff Amy in Atlanta; Melinda Deslatte in Baton Rouge, Louisiana; Morgan Lee in Santa Fe, New Mexico; Mark Scolforo in Harrisburg, Pennsylvania; and AP economics writer Christopher Rugaber, in Washington, D.C.
This story was originally published July 1, 2020, by Kaiser Health News.
