


According to the World Health Organization, global all-cause mortality from illness is highest for heart disease (9 million) and stroke (over 6 million in 2019). The fourth leading cause of death — lower respiratory illnesses like pneumonia, flu, and tuberculosis — has claimed approximately 2.6 million lives for the past 20 years, consistently.
Even before COVID-19 arrived on the scene, highly infectious respiratory disease was one of the primary public health threats legislators faced. For approximately 10 -15 years, research has been focused on preventive vaccination, rather than on treatment and improvement in public health infrastructure at the point of care.
There is, frankly, not a lot of evidence that this strategy has been successful.
The mortality and infection rates for seasonal influenza, for example, have remained more or less the same for two decades. The influenza vaccination industry has grown significantly, however. The WHO has become a pivotal institution involved in global surveillance and classification of influenza virus mutations each year. From the WHO’s determination of the three most prevalent strains, pharmaceutical companies produce a product tailored (theoretically) to each flu season and roll it out to government agencies.
The steps of government marketing approval, sales to health care providers and citizens, and stockpiling happen largely without incident. If new types of influenza-like illness emerge and begin to infect humans, such as H1N1 or swine flu, existing production structures are easily adapted for manufacture of vaccines against the newly emerging threats. This is one of the main arguments for maintaining the influenza vaccine production infrastructure, even in years where there might be low demand for, or even low efficacy of, a given product.
What gets lost in the shuffle is any hint that local structures delivering medical care to the substantial numbers of people affected (3-5 million severe cases globally, causing up to 650,000 deaths annually, with seasonal influenza) are impacted in any positive and meaningful way — for example, by helping doctors improve treatment outcomes for patients.
Although the burden of efficacy proof for preventive vaccination should lie with producers, it does not. Corporations essentially police themselves, delivering carefully culled datasets and documentation to agencies for approval shortly before the next influenza season looms. This poses a dilemma for elected officials in charge of public health: to take the time to look into the data more thoroughly, or to question its validity, is to risk being caught unprepared with that potentially preventive vaccination (and blamed!) when the next respiratory illness invades the airspace of a given territory.
The problem of infectious viruses too small to be seen without a microscope using computer-aided electron wave technology to magnify them several thousand times is highly technical, to put it mildly. Once a vaccine has been developed and approved, there is little incentive to keep monitoring efficacy or impact on disease prevention. With diseases like influenza, comparison of each season’s vaccine formulation against circulating strains is practically impossible and of little value for the following year.
Legislators and leaders are threatened with damage to entire economies and the tax bases needed to maintain government services for citizens — if, for example, enough of their constituents become too ill to work, or hospitals become overburdened and fail.
At the same time, there is incentive for government regulators and manufacturers alike to downplay or fail to follow-up on safety concerns. Headlines like: “NIH ‘Very Concerned’ about Serious Side Effect in Coronavirus Vaccine Trial” hint at danger. Serious damage to formerly healthy individuals like the post-vaccination transverse myelitis documented here often gets lost or ignored by a 24-hour news cycle, which is not designed to take up the slack where government regulators fail to adequately hold corporations responsible for the safety of study subjects.
Pharmaceutical companies, by releasing preliminary data about “interim analyses” before regulatory agencies release reports on the final data like these Moderna or Pfizer FDA dossiers, are essentially governing by press-release. They have leveraged the media apparatus to trumpet claims about an “efficacy rate of 95%” that go entirely unchallenged.
Using the Pfizer document, I finally resorted to testing my memory of cross-multiplication to determine percentages. On p.17, the ‘final efficacy analysis” was apparently conducted whenever 170 people in the study had caught COVID. However, on p.32, there is mention of a “primary efficacy endpoint” which muddies the water a bit. Of the 21,669 people who were vaccinated, 50 got COVID after Dose1: with 39 of them infected sometime between Dose1 and Dose2; 2 infected a few days after Dose2; and nine who were infected seven or more days after Dose2. The analysis presented to the public seems to be based on those nine that both doses of vaccine failed to protect.
The 50 vaccinated people who got COVID comprised .23% or about a quarter of a percent of the total vaccinated group of 21,669. If you choose to count only the nine, that’s only .04%. But in the placebo group 275 (1.27%) of 21,686 people got the disease. It therefore appears that the vaccine was about 1% more effective than the placebo, or 1.23% if you only count the nine who were vaccinated with both doses before getting COVID.
Medical studies are designed to look at both efficacy and safety. Yet only 2,238 of the study subjects were included in something called the “reactogenicity subset of the safety population aged 18 to 55 years.” (P.35, Table 17). There are several pages of further “subset” analyses, using various age groups, etc. I searched the entire report but could not find a comprehensive listing of safety data for all participants.
Without complete data on how many of the more than 40,000 people serving as vaccinated and placebo subjects had fatigue, headache, chills, nausea, vomiting, etc., all we have are relatively meaningless numbers…
…Unless we use the same tactics pharmaceutical companies are using, and extrapolate. This “reactogenicity subset” of 2,238 people is approximately 1/10th the size of the full data-set of 21,669 vaccinated subjects. After vaccination, 1,085, or almost half, were fatigued. This would be over 150 million people if everyone in the U.S. were vaccinated.
One could argue that needing a nap is not a good reason to decline vaccination against severe disease. But what about the 959 (42%, 9,100 of full data-set, 134 million if all Americans were vaccinated) who had headache, 14% of whom had a bad headache? What about the apparently tiny 1.2% of the subset who vomited?
Extrapolated to the full U.S. population, must we expect that 3,840,000 people may vomit if the entire country is vaccinated? Serious systemic side effects such as muscle pain (reported by 21%) and new or worsened joint pain (11%) may also be harbingers of autoimmune disease and other lasting systemic damage, that could emerge long after vaccination.
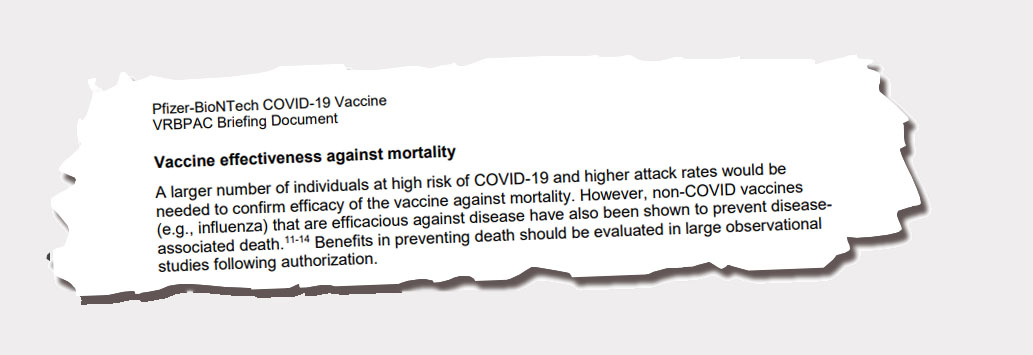
Vaccines have been shown to worsen some cases of subsequent infection, a phenomenon called antibody-dependent enhancement. And the best part? There’s no proof that vaccination protects against death from COVID. According to the Pfizer/FDA report (p.48) “A larger number of individuals at high risk of COVID-19 and higher attack rates would be needed to confirm efficacy of the vaccine against mortality.”
Economic modelling done by professional statisticians is often used to claim that the ounce of prevention provided by a vaccine is much better than the pound of cure that well-funded hospitals, fully staffed with professional nurses and doctors, using effective pharmaceutical remedies, can provide. But is this actually true?
Genevieve Diamant PhD of Hampton is a former medical writer for an international pharmaceutical company that specializes in vaccines.