


The patient was dying. Her medical chart showed she had an advance directive that would explain the type of end-of-life care she wanted, but it had been written eight years earlier.
The woman’s son said she’d told him recently that she wanted to get better. To him, that meant that the advance directive shouldn’t apply — a view one of the woman’s other children opposed.
The hospital’s risk management department told the woman’s doctors to do what they needed to do to keep her alive and talk to the probate court when it opened Monday, recalled Dr. Joanne Kuntz, one of the physicians involved in the woman’s care.
“Which is really not how you want to provide health care,” said Kuntz, who spent two decades as an emergency room physician and is now director of palliative services at UConn Health.
People who provide emergency medical care say situations like this are common: A dying patient’s wishes aren’t known or are in dispute, leaving her relatives to agonize over what to do. Or a terminally ill patient comes to the hospital with no record of his treatment wishes and ends up getting more aggressive care than he’d wanted.
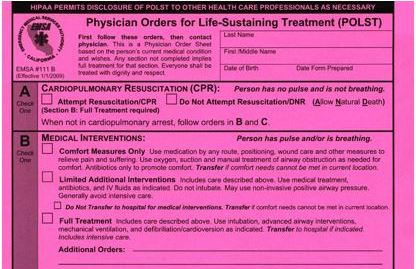
Kuntz and others say there’s a better way: A process for terminally ill patients to discuss their options with a health care provider, determine what sort of end-of-life care they want, and document it in a form that would serve as a medical order for emergency responders, physicians and others in the health care system to follow. It would make clear patients’ wishes: Would they want CPR? A feeding tube? Treatment solely to relieve pain and suffering, limited medical interventions such as antibiotics and fluids if needed, or full treatment that could include intubation and intensive care?
A proposal now under consideration in the state legislature would create a pilot program for the process, referred to as medical orders for life sustaining treatment, or MOLST. It would be voluntary and available only to patients approaching the end stage of a serious “life-limiting” illness or with advanced, progressive frailty.
Talk of end-of-life issues in the legislature this year has largely focused on a high-profile and controversial bill that would allow physicians to prescribe lethal doses of medication to mentally competent, terminally ill patients.
But many people believe the MOLST bill is the one that has a good chance of becoming law. It has the support of Gov. Dannel P. Malloy, who has not taken a position on the assisted suicide bill.
And it has the backing of two groups that fought a similar measure last year out of concern that the medical orders could be used to deny care. Members of Second Thoughts Connecticut, an organization representing people with disabilities, endorsed this year’s proposal because it includes safeguards they say address their concerns, although they’re still cautious about the model.
Similarly, the Connecticut Catholic Public Affairs Conference opposed the proposal last year but supports the concept of this year’s bill.
The proposal was developed through a lengthy process led by the state Department of Public Health that included people with disabilities.
“We think it’s going to be really cutting edge, in fact a model that other states ought to aspire to,” said Catherine Ludlum, a member of Second Thoughts Connecticut, who fought the previous bill but helped develop this year’s proposal.
A delicate topic
More than 40 states have similar medical orders programs in place or efforts under way to create them. But end-of-life care has historically been a politically delicate subject.
In 2009, as Congress debated proposals that became the federal health law now commonly known as Obamacare, opponents used the term “death panels” to describe a provision that would have paid doctors to counsel Medicare patients about end-of-life treatment options. The provision never made it to the final bill.
And this year’s assisted suicide proposal has produced strong reactions. Supporters, who call it “aid in dying,” say it’s a matter of compassion and peace of mind for people facing terminal illnesses, while opponents warn it could leave people vulnerable, particular those who are elderly or have disabilities.
Asked about the MOLST proposal, Tim Appleton, who is directing the campaign for the aid in dying bill for the advocacy group Compassion & Choices, focused instead on the bill his group favors, citing a recent Quinnipiac University poll that found broad support for assisted suicide in the state.
“The great thing about the Quinnipiac poll, and the great thing about organizing for this issue in the state, is any number of different end-of-life conversations are happening, not only at the state Capitol but in the media as well, and [in] families all around the state as a result of the reporting done on end-of-life issues and end-of-life choice,” Appleton said.
Some MOLST supporters have described their proposal as an alternative to assisted suicide, while others have tried to distance the two concepts, noting that the medical orders would allow patients to undergo a natural death but wouldn’t allow them to end their lives.
Limits of advance directives

The concept behind developing medical orders for end-of-life care began in Oregon close to 25 years ago.
“What the recognition was was that people were being given treatment that they either didn’t want or might not have been appropriate for them, especially when they were transitioning from one type of health care facility to another,” said Paul Drager, an attorney who has been involved in establishing similar programs in several states.
Connecticut law allows people to complete advance directives that explain what type of care they would want and designate a person to make health care decisions if they can’t.
But advance directives don’t carry the force of medical orders, and research suggests they’re often misinterpreted by medical personnel. They’re often vague and completed without a medical expert. And people who work in emergency rooms say it can be difficult to know if an advance directive is still in effect or if it’s been amended or revoked.
Supporters say MOLST would complement advance directives by turning them into medical orders tailored for people near the end of their lives. And they would be designed to be easily transferred across medical settings.
Many states use bright-colored paper to make the forms easily identifiable. In Oregon, people are encouraged to put their forms on their refrigerators, and emergency responders are trained to look there. Some states suggest people keep them in medicine cabinets. And some have registries that store the orders centrally, said Amy Vandenbroucke, executive director of the National POLST Paradigm, which promotes the programs. (Many states use the acronym POLST, or physician orders for life sustaining treatment.)
Without a formal process or document, Kuntz said, a patient could have a meaningful conversation with a doctor at St. Francis Hospital and Medical Center in Hartford about the sort of care he or she would want. “But if they show up at UConn sick, we have no way of knowing or following through with whatever conversation they may have had at the hospital across town,” she said.
When the risk is not enough care

Officially, MOLST is neutral on what people choose. Someone with the orders could ask for aggressive life-saving care or comfort measures only, or something in between.
But some people with disabilities see the process as largely aimed at limiting treatment — a particular concern because many people with disabilities say they’re at greater risk of not being given the same life-saving options other people receive.
Ludlum and Stephen Mendelsohn, another Second Thoughts Connecticut member who was part of the group that developed the proposal, consider the medical orders programs in other states problematic. Some don’t require a patient’s signature to verify that he or she participated in developing the orders.
In some states, people with life expectancies of up to five years can create the orders, which Ludlum said increases the possibility that orders created with a particular condition in mind could be used in responding to unforeseen situations like a car accident or a severe allergic reaction.
Ludlum, who uses a feeding tube and breathing support, said it’s also important to ensure that people are fully informed about the choices, rather than given biased information that presents being on a ventilator or feeding tube as horrible.
“It’s very important to understand that this whole process needs to not become a checklist,” she said. “It needs to be a productive and useful conversation between the patient and the health care practitioner.”
Connecticut’s proposal requires that a MOLST be signed by the patient or a legally authorized representative. Before requesting the signature, health care providers would be required to discuss with patients their goals for care and treatment, and the benefits and risks of different methods for documenting their wishes for end-of-life treatment.
It also requires health care providers who want to write the orders to receive training on the importance of talking with patients about personal treatment goals, methods for presenting choices without directing people to a particular option, and awareness of factors that could affect the use of MOLST, including race, ethnicity, age, gender, socioeconomic status, mental illness and disability.
Although Second Thoughts Connecticut is supporting the bill, Ludlum said it’s with caution.
“I think we’re always going to be a little bit cautious because the trainings they’re going to have in how to use this are really key,” she said, adding that the process won’t work if the trainings don’t help health care providers overcome their own biases and embrace their patients’ choices.
Michael C. Culhane, the Catholic Conference’s executive director, said the organization supports the legislation in concept, but he would like it to place more emphasis on including family members and trusted friends in the process — something he said could be achieved when regulations are written for the pilot program.
“If we can ever get to a point where patients can actually trust that those kinds of conversations are intended to be a support and form of advocacy for them, and not a way to withhold care from them, society really benefits,” said Dr. Jewel Mullen, the state’s public health commissioner.
“Because then we don’t end up having people wonder, when the conversation comes up at a critical moment, maybe left to a family, people don’t have to start wondering, ‘Is it that they don’t want to treat me?’ Or people don’t have to feel stuck saying, ‘I want this therapy stopped for my loved one, but the doctors don’t feel like they can.’”
