




Would you buy a health plan that covered fewer hospitals and doctors if the premiums were 10 percent less?
Officials at Connecticut’s health insurance exchange are betting some customers would welcome that tradeoff. The marketplace’s board recently voted to loosen the requirements on the size of insurance provider networks on plans sold to its customers starting next year.
So-called narrow network plans have not gained much traction in Connecticut. It’s been standard in recent years for all insurers to cover every hospital in the state, for example. But some, including the state’s insurance commissioner, think narrower-network plans could become more prominent as health care costs, and insurance premiums, continue to rise.
“I think there is an opportunity for real cost savings,” Insurance Commissioner Katharine L. Wade said. “But the thing that’s really important, and we want to make sure, is that people are fully understanding the decisions they’re making. We don’t want people to make decisions on price and not understand that there may be limitations on that choice.”
Some in health care see narrow networks as a reflection of economic reality.
“On the one hand, everyone wants to pay a lower premium. On the other hand, in a perfect world, you don’t want your choices constrained,” said Dr. Rocco Orlando III, senior vice president and chief medical officer for Hartford HealthCare, the parent company of five Connecticut hospitals. “You can no longer have it both ways. You’re either going to have unconstrained choice and pay more, or you will accept some reduction in your options, and that’s going to be kinder to your wallet.”
But others see narrow networks as a poor option. The Connecticut State Medical Society called the recent move by the exchange, Access Health CT, to allow narrower networks “bewildering,” and warned that it could hurt patients’ access to care.
“This Access Health CT decision will give the health insurance plans a free pass to create insurance products which offer only deeply restricted access to medical treatment,” the medical society said in a statement. “These narrowed networks also further exacerbate the trend of cost shifting to employers and consumers.”
How they work
Why would a narrower-network plan cost less?
It’s because insurance companies could seek to pay lower prices for care to hospitals and other health care providers, in exchange for sending them more patients. An insurer could opt to contract with only one of the two general hospitals in Hartford, for example. That hospital would then get lower payment rates, but a larger share of the patients covered by that health plan.
In many parts of the country, health insurance exchanges set up under the Affordable Care Act have already included plans with narrow networks. But Connecticut’s exchange has limited the ability of insurers to reduce their networks. Currently, plans sold through the exchange must cover 85 percent of the providers covered by the insurer’s broadest network.
But with concerns about the price of premiums, the exchange’s board voted last month to eliminate that standard. Insurance Department Actuary Paul Lombardo told board members that insurers have said narrowing their networks could lead to premium savings between 5 and 10 percent.
State Healthcare Advocate Ted Doolittle said at the time that moving to narrow networks could be viewed as anti-consumer. But he said he supported the change because the networks would still be subject to an insurance department review, and because allowing narrower networks could put price pressure on health care providers, helping to target unsustainable health care cost growth. (The board voted in February to have the change in network standards be in effect for only two years, something Doolittle requested as a way to allow the concept to be revisited if there are problems. But the board voted at a subsequent meeting to lift that limit.)
Insurer networks on the exchange would still be subject to a review by the insurance department that takes into account, among other things, the number of health care providers overall and in particular specialties included in a plan’s network, how many providers accept new patients, and appointment wait times.
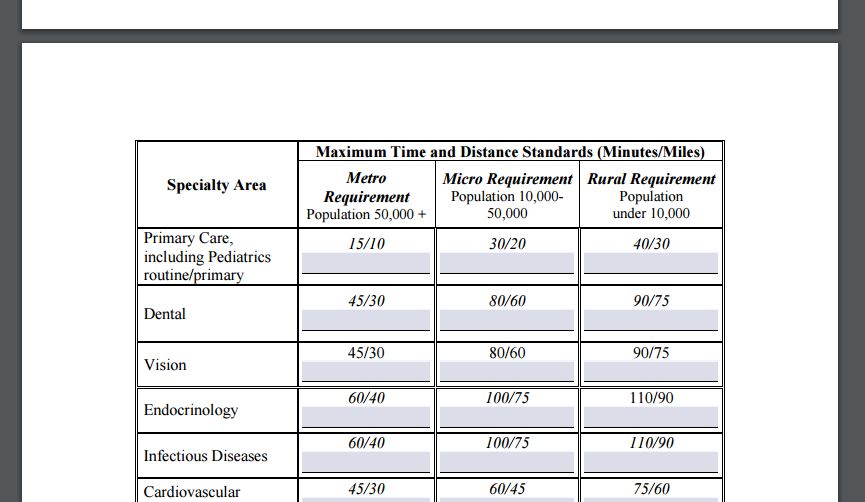
The network adequacy review includes standards with maximum travel time and distance for primary care and specific specialties. For example, 90 percent of members in a metropolitan area with at least 50,000 people would have to be able to get to an in-network primary care provider within 15 minutes or 10 miles, to a hospital within 45 minutes or 30 miles, and to a cardiology specialist within 45 minutes or 30 miles. The times and distances are larger for those in areas with smaller populations.
Insurers praise flexibility; docs see concerns

The exchange’s move to allow narrower networks drew applause from the two insurers that sell insurance through Access Health.
“It is our mission to deliver affordable, quality care. This change affords carriers more options to develop products at various price points to meet consumers’ needs,” Anthem Blue Cross and Blue Shield said in a statement.
The company said it is still evaluating its products for 2018 and hasn’t determined if it will offer a narrow network plan.
Eric Galvin, ConnectiCare’s president and chief operating officer, said the change would allow the company to offer different types of products. Still, he noted, while it might allow for competition between providers in some areas, there are other parts of the state without that competition, such as New Haven, where Yale-New Haven Hospital is the only hospital.
Hartford HealthCare – the parent company of Hartford, Backus and Windham hospitals, The Hospital of Central Connecticut, and MidState Medical Center – is already part of one limited network product that covers its providers as well as smaller hospitals that are part of the Value Care Alliance – including Griffin and Middlesex hospitals. That plan is offered by Aetna to employers.

“There is interest in the market to do some of these, and so we’re just looking at it as simply a reality of having a variety of insurance products available in the market,” Orlando said.
But the prospect of narrower networks has provoked intense opposition from the state medical society.
Matthew Katz, the organization’s executive vice president and CEO, noted that many patients in exchange plans already have high deductibles, meaning they must pay thousands of dollars toward the cost of their care before their plan begins covering the cost. Many plans have higher deductibles for out-of-network care, and Katz said if patients struggle to find doctors who participate in their insurance networks, they will face even higher out-of-pocket costs.

“Insurance becomes illusory because you’re really never having the insurer kick in,” he said. The real way such plans save money, he said, is by leading people to put off care.
If patients have less choice in which providers they can see, he added, they could face longer wait times for care.
And Katz said there are significant concerns about the criteria insurers would use to determine which doctors to include in their networks.
Is there an appetite?
Tim Tracy Jr., a Fairfield insurance broker and president of the Connecticut Chapter of the National Association of Health Underwriters, said he thinks there’s likely to be an appetite for narrow network plans if they come with lower premiums than plans with more robust networks. While some people will always want the option of going to any hospital or specialist, some will be happy to limit themselves to certain providers.
“It’s definitely, I think, a viable solution for many people. It’s just you want to make sure you know what you’re getting,” he said.
Education is key for anyone considering narrow network plans; customers need an easy way to find which providers are covered, Tracy said. That means knowing not just to ask if a doctor takes a certain company’s insurance; some doctors take only certain plans offered by an insurer, so patients must ask if a provider accepts their specific plan.
“Oftentimes we can see a lot of confusion,” Tracy said.
Darren Walsh, who owns a health benefits consulting firm in Fairfield, is less convinced people will find narrow networks appealing.
Many people already have deductibles in the range of $5,000 or $10,000 per year, on top of premiums that can top $20,000 for a family, he noted. For them, he said, the purpose of insurance is “in case you get hit by the proverbial bus – cancer, major surgery, some debilitating chronic illness,” the sorts of things that can cost tens of thousands of dollars.
“And then you want access to have the very best hospitals and specialists in the region,” he said. “Why would you buy a product, a narrow network, that wouldn’t have those doctors?”
Galvin, from ConnectiCare, said the appeal is likely to depend on who is, and isn’t, in the network.
“At the point of purchase, I think people are very willing to do it, because they’re staring at that premium, and they’re staring at potentially the difference in premium between a very, very broad, open choice type of a network, and a limited, more narrow network,” he said.
“If your doctor is in the network, you’re generally agnostic to it,” Galvin added. “If your doctor is not in the network, then I think you’re still able to switch, but it’s a much harder decision to make.”