



Telehealth use expanded greatly with the start of the COVID-19 pandemic in 2020. Until now, however, little has been known about the results for patients who used telehealth during the pandemic as compared to those who received medical services without telehealth. A new study by FAIR Health sheds light on this issue in Connecticut, with particular attention to differences in treatment in areas with greater minority populations.
Funded by a generous grant from the Connecticut Health Foundation, we conducted the study by delving into our repository of private healthcare claim records—the nation’s largest such database.

The data used in the analysis spanned over two years, beginning at the start of the COVID-19 pandemic in March 2020 and continuing to September 2022. The study population comprised 1,066,140 commercially insured patients who were residents of Connecticut and received medical services in that period. The population included 429,634 patients who received at least one telehealth service and 636,506 patients who received only in-office care.
As part of the study, we did an in-depth analysis of seven of the most common and well-known health conditions treated via telehealth in Connecticut: anxiety and other nonpsychotic mental disorders, mood (affective) disorders, COVID-19, acute upper respiratory infections, hypertensive diseases, diabetes mellitus and substance use disorders.
Overall results
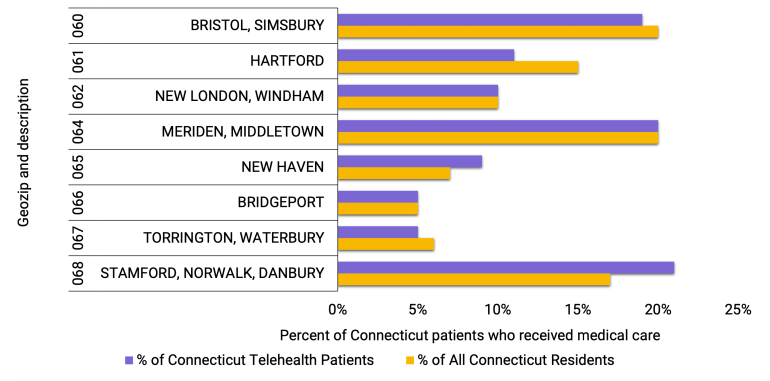
We divided into “geozips,” geographic regions typically corresponding to the first three digits of a zip code. In most of the eight geozips in Connecticut, the share of patients using telehealth was fairly similar to that using all medical services. The two main exceptions were geozip 061 (Hartford), which had a lower percentage of patients using telehealth, and geozip 068 (Stamford, Norwalk, Danbury), which had a higher percentage of patients using telehealth.
Overall, in Connecticut, patients who used telehealth were more likely to be hospitalized and have emergency room (ER) visits than patients who used only in-office care, and that likelihood was higher for those who had more hospitalizations or ER visits. For example, patients who used telehealth were 1.17 times as likely to have any hospitalization, but 3.94 times as likely to have six or more hospitalizations. It is beyond the scope of this study to determine whether telehealth treatment or differences in the patients who select telehealth care led to the different results.
We also compared patients who used telehealth and those who did not to see which group had more visits than average—including telehealth visits, in-person visits, ER visits and hospitalizations—and which group had higher total “allowed amounts” than average for all the medical services they received. (An allowed amount is the total negotiated, in-network fee paid to the provider under an insurance plan.) Connecticut telehealth patients were almost 15 times as likely as those who did not use telehealth to have more total visits than average, and over 10 times as likely to have a higher allowed amount sum than average.
Condition-specific results
For all seven health conditions, greater racial and ethnic diversity in an area of Connecticut (as measured by a smaller percentage of white people) correlated with higher average numbers of hospitalizations and ER visits for both patients who used telehealth and those who did not use it. For six out of seven conditions, the differences among the three different population groupings (geozips that are 26 to 50 percent white, 51 to 75 percent white and 76 to 100 percent white) were statistically significant.
The percentage of white residents in an area includes those identified by census data as white, as distinct from Black, Hispanic, Asian and other. The three geographic groupings included in this study are all geozips that are 26 to 50 percent white, 51 to 75 percent white and 76 to 100 percent white. Because no Connecticut geozip is less than 26 percent white, the proportion 0 to 25 percent white is not included in this study.
For all seven health conditions, patients who used telehealth had higher average numbers of hospitalizations and ER visits than those who did not. The difference was especially pronounced among patients with diabetes mellitus and hypertensive diseases. Patients who used telehealth for these conditions had approximately double the average number of hospitalizations and ER visits as patients who did not use telehealth.

For two behavioral health conditions (anxiety and other nonpsychotic mental disorders, and substance use disorders), higher average overall costs for treatment were associated with patients who used telehealth. By contrast, lower average costs were associated with patients who used telehealth for two infectious conditions (acute upper respiratory infections and COVID-19).
For the two behavioral health conditions, average total allowed amount per person was higher for patients who used telehealth than those who used only in-office care across each of the eight geozips in Connecticut and across the state as a whole. For the two infectious conditions, average total allowed amount per person was lower for patients who used telehealth than those who used only in-office care in all eight geozips and statewide. Telehealth for the remaining three conditions varied by geozip and statewide.
Visits for patients who used telehealth for anxiety and other nonpsychotic mental disorders were the most likely to have higher-than-average total allowed amounts for all treatment received for that condition. Such patients also had more anxiety-related visits than average, which may indicate greater adherence to treatment. Visits for patients who used telehealth for COVID-19 were the least likely to have higher-than-average total allowed amounts.
For treatments that included telehealth, substance use disorders were the condition with the highest likelihood of having more visits than the average number of visits. Acute upper respiratory infections were the condition least likely to be associated with more visits than average when treatment included telehealth.
It is beyond the scope of this study to determine whether the increased visits, costs, ER visits and hospitalizations generally associated with telehealth in Connecticut in 2020-2022 were necessary or unnecessary, or whether there was a causal relationship between telehealth and the measured results. For example, with behavioral health conditions, a greater number of visits may indicate greater adherence to recommended treatment for those conditions. Similarly, increased visits noted for patients with diabetes and hypertension—both conditions that disproportionately affect people of color—may indicate increased remote monitoring.
We hope that other researchers will build on the findings reported in this study to learn more about the effects of telehealth, particularly on reducing barriers to care. We also hope that this study will be of value to other healthcare stakeholders in Connecticut and nationwide, including payors, providers, policy makers and patients.
Here is the complete study.
Robin Gelburd is the founding President of FAIR Health, a national, independent nonprofit organization working in healthcare cost transparency, data analytics and benchmarks.


