


The role of socioeconomic class on cardiovascular health outcome cannot be overemphasized. A child born to parents with college or advanced degrees will likely live an average of ten years longer than another child in the same city whose parents are without high school diplomas.
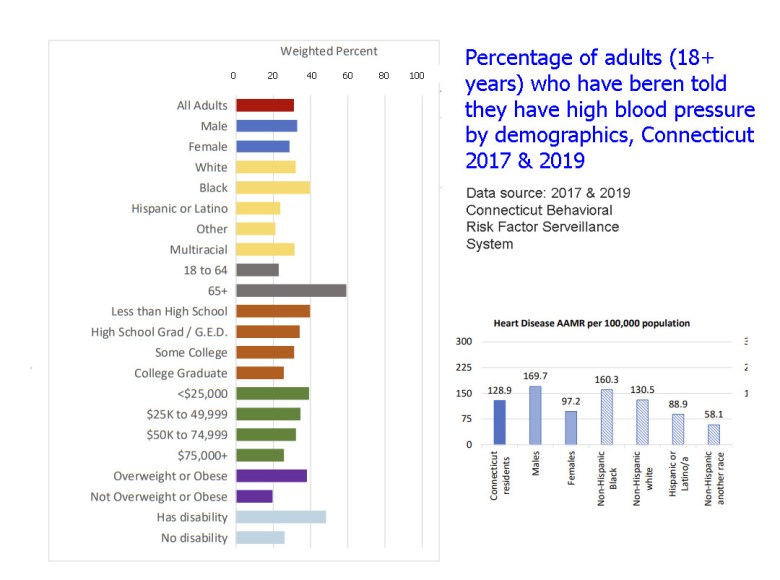
In Connecticut, adults with lower educational attainment are significantly more likely to be diagnosed with cardiovascular disease. In 2021, the state’s age-adjusted heart-disease death rate was 137.6 per 100,000 — a figure that underscores the structural gap in heart outcomes. Essentially, both hearts are on different trajectories largely due to the difference in socioeconomic status.
The general school of thought in the United States is that cardiovascular problems are largely ascribed to dietary patterns, lifestyle and to some extent, family history. The unspoken truth however is that the prognosis of cardiovascular health is often set even before a patient’s first appearance in a clinic.
Heart disease remains the leading cause of death in the United States. Despite advancements in treatment and medical innovation, it is surprising that there is still a rise in the burden of cardiovascular mortality as reported by the American Heart Association. Moreover, this burden is highest among individuals without college degrees. According to research, adults with less education are nearly two times more likely to die from heart disease than those with higher educational attainment. These outcomes represent the impact of social and economic status on health and life expectancy.
Social and economic factors influencing health outcomes have been described by public health researchers as “causes of causes.” As sociologists Bruce Link and Jo Phelan argued, diseases and social gradients are inseparable because resources like education, income, housing and power that significantly impact health are unevenly distributed. There is a direct correlation between socioeconomic status and health outcomes; the more advantages one has, the better access to opportunities to reduce cardiovascular risks. Those without these advantages are victims of food insecurity, unsafe neighborhoods, lack of insurance limiting access to preventive care.
Using blood pressure as a case study, an individual with a college degree is more likely to have health insurance and access to primary health care compared to an individual of the same age without a college degree. The individual with better access to health care benefits from regular screening and early detection of hypertension and other comorbidities. The prognosis of chronic diseases like hypertension is largely dependent on the stage of detection before the commencement of treatment. Another individual, for example, a single mother working two jobs without paid time off may be unwilling to take to take out time to see a doctor due to fear of losing wages or job termination. The longer her blood pressure goes untreated, the more likely she develops cardiovascular complications.
Educational disparities are not just a reflection of individual opportunity, they show how power and policy shape health. Environmental hazards, fast-food outlets and insecurity are more likely to be prevalent in communities with lower average education levels. These stressors play a role in contributing to the prevalence of cardiovascular problems like hypertension because disease processes are influenced by biological and environmental factors. Stressors cause the release of certain hormones like cortisol that play a role in the pathophysiology of hypertension.
The consequences of these disparities are evident here in Connecticut. In New Haven, there is a striking difference in neighborhoods a few miles apart not only in life expectancy but in cardiovascular outcomes. According to the Connecticut Department of Public Health, heart diseases are the top causes of death in the city however, this burden is highest in neighborhoods with lower household income and educational status. This difference is not due to chance, it is as a result of structural disparities, reflecting years of disinvestment and educational inequality—the true heart disease epidemic hiding in plain sight.
This is not to disregard the significant role of personal choices on health outcomes. Diet, exercise and smoking all influence cardiovascular risk and individuals have the responsibility of enforcing lifestyle modifications to improve their outcomes. However, these choices are not made in isolation, they are a reflection of environmental realities and health policies. A neighborhood with sidewalks encourages jogging as opposed to one with a high incidence of gun violence. It’s also easier to purchase and consume vegetables if the nearest grocery store isn’t three bus rides away. It’s easier to educate people about personal choices, however, we shouldn’t blame them for predictable outcomes if those personal choices are systematically limited by their environment.
Moving upstream is an effective strategy if the goal is to reduce the burden of heart disease. This involves investment in early-childhood education, equitable housing policies and guaranteeing living wage. These interventions may not be captured within the scope of preventive cardiology but in reality, offer the most effective heart disease prevention strategy. Further research has shown that for every additional year of education, the risk of heart disease and stroke is lower. This is a reflection of how impactful universal access to quality education can be on cardiovascular health.
Policies will drive the next major breakthrough in cardiovascular health. Expanding access to affordable housing, strengthening living wage laws, investing in early childhood education, and ensuring universal health coverage are the kinds of political reforms that can truly lower heart disease risk.
We cannot stent our way out of structural inequality. Heart diseases may be measured using anatomical and physiological criteria but they are made in systems.
Micah Okwah MD attends the Yale School of Public Health.


