


I am a board-certified family physician, recently retired from direct patient care after 42 years in clinical practice. I truly loved building and sustaining relationships with patients which allowed me to contribute to their well-being and health over many years.
My patients’ cultural and ethnic diversity always challenged me to listen to their needs and respect their backgrounds and values — values that guided me in the application of the medical standards of care to their identified healthcare issues. Often there is more than one approach to diagnose and treat a medical issue and the success of providing their care is doing so through the skill of “shared decision-making.”

Throughout my clinical career I have always felt secure about the role our state and federal governments have in supporting and promoting our health care delivery system…until now.
To borrow a phrase from the long cherished “Star Wars” series–I feel a “disturbance in the force.” All my life I believed that our society and our government valued “the Common Good” above all else. This simple yet supremely powerful statement was first expressed in ancient Greece, by Aristotle and other philosophers, over 2000 years ago. It was interpreted to mean that the purpose of the city-state/government was to “help citizens live a good and flourishing life, to promote the welfare of the whole community.”
Today “the common good” generally means: the social conditions, institutions and resources that allow all members of a community to flourish and pursue their wellbeing.” A strong primary care system is a common good because everybody benefits when communities have accessible, preventative and coordinated healthcare whenever and wherever it is needed.
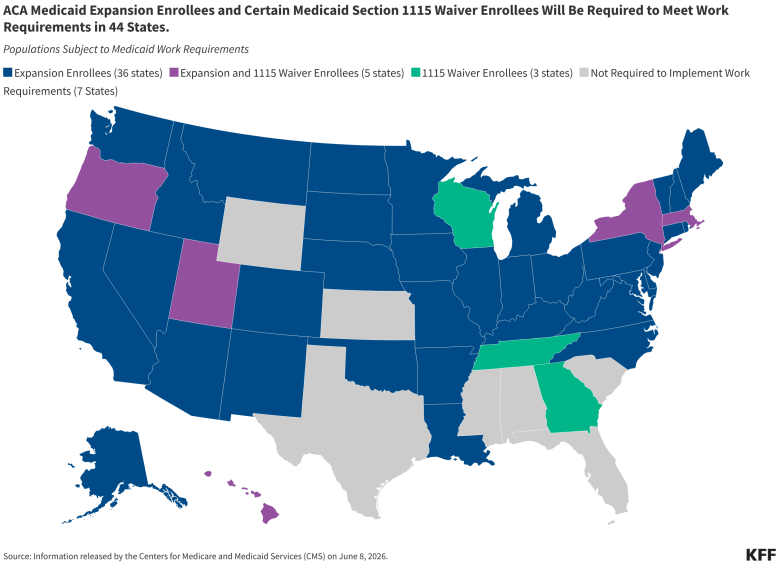
One alarming and expected outcome from the One Big Beautiful Bill, according to the Congressional Budget Office, is that immediately five million people could lose Medicaid coverage because of the work-reporting requirement, rising to 7.8 million by 2034, and most would become uninsured rather than move to employer-sponsored insurance.
Studies of prior Medicaid work requirement programs found NO meaningful increase in workforce participation. To add serious insult to injury on June 1 the federal government announced an interim final rule defining “medical frailty.” In Connecticut alone 110,000 citizens are expected to lose state Medicaid coverage as a result of this further tightening of eligibility.
The issue is that states must now prove that the condition “significantly impairs” a person from fulfilling work requirements. According to Connecticut Hospital Association vice-president Mark Schaefer, “That two-pronged test –diagnosis AND impairment –is seismic in its effect on the coverage loss projections”. According to Barton Reeves, Connecticut’s social services commissioner, “ NO ONE in ANY state agency…across the country has medical staff in place with the subject matter expertise to make that determination.”
In brief, this encompasses those with:
- physical, intellectual and developmental disabilities
- blind or disabled
- disabling mental disorder
- serious or complex medical condition
- substance use disorder
What this will mean for those citizens dropped off their state Medicaid roll:
- delayed primary care visits
- reduced access to preventative services
- difficulty affording medications
- increased medical debt
- greater use of emergency room care when underlying illness becomes more severe.
Combining Medicaid and Affordable Care Act (ACA) changes, CBO estimates that 11-12 million citizens could be uninsured by 2034. The House Republican’s budget reconciliation legislation would cut assistance that helps children in families with low incomes get enough to eat. The Supplemental Nutrition Assistance program (SNAP) would receive the largest cut in its history, nearly $300 billion through 2034. Expanding the work requirements would cut SNAP benefits for another 1 million children.

To summarize, there is evidence that political rhetoric, leadership style and the broader political climate can affect mental health and, indirectly, physical health. Studies have found that periods of intense political polarization can be associated with:
- increased anxiety and stress
- sleep disturbances
- elevated blood pressure
- worsening cardiovascular risk
- exacerbations of depression, irritable bowel syndrome, headaches and chronic pain.
Very importantly, many of the health effects of social and political environments were recognized only years/decades later. The term “social capital” has been defined as “features of social organizations” such as norms, networks and trust that facilitate coordination and cooperation for mutual benefit.”
Examples in community health include -faith communities supporting sick members, families providing caregiving, and volunteer organizations filling gaps in social services.
These activities are truly Community-Level Health Assets, much as blood pressure control is an individual-level health asset. Public health researchers have linked “Higher Social Capital” to:
- Lower mortality rates
- Better self-reported health
- Lower depression and suicide rates
- Greater community resilience during disasters
Just as health depends on more than medical care, societal well-being depends on more than individual success. Communities rich in social capital generate trust, belonging, and shared purpose—the very conditions that allow both people and institutions to prosper. Protecting and strengthening these connections may be among the most important investments we can make in the future health of our nation.
H. Andrew Selinger M.D. is an Associate Professor of Family Medicine, Frank H. Netter MD School of Medicine at Quinnipiac University
