



Early one recent morning, an inmate at the state’s lone women’s prison gave birth in her prison cell.
That incident – as well as large budget cuts, a lack of outside oversight and a history of complaints – have fueled concerns among some legislators and civil rights groups about the quality of medical and mental health care being provided to inmates.

Care for the 14,000 inmates the state incarcerates on any given day is slated to undergo significant changes in July when the Department of Correction takes over managing it from UConn Health. However, some involved say changing management won’t necessarily address issues that have led to their concerns.
Mental health care is a particular worry because most of the inmates eventually will be released.
“They have a line of people waiting there for care. A lot of the mentally ill are dumped in prison,” said Deborah Shelton, editor of the Journal for Evidence-Based Practice in Correctional Health and professor emeritus at the UConn School of Nursing, whose expertise is inmate health.
On Feb. 22, one-quarter of the inmates in the state’s prisons – 3,486 people – had a mental health disorder that requires regular treatment. Add in the 5,378 inmates who have mental health issues but have been determined to not currently need treatment, and two-thirds of those the state locks up have a history of mental illness.
Quality care?
Since 1997, UConn’s Correctional Managed Health Care (CMHC) has run health care for the state’s prison system under a contract with the correction department. That contract was worth $140 million last year. While it required quality-assurance measures, several were not followed.
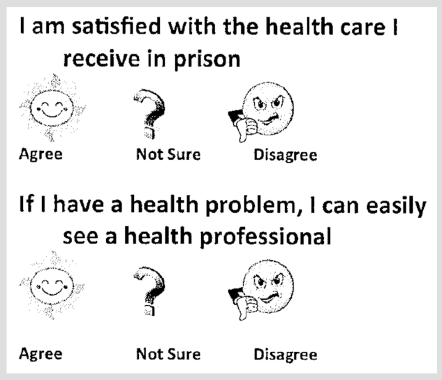
For example, after a survey of inmates identified concerns about the health care they were receiving, CMHC didn’t follow up to track progress.
The survey results – published in the Journal of Correctional Health Care in 2014 – showed one-quarter of those surveyed were satisfied with the care they were receiving. Just over half responded they were not able to easily see a health care staff member if they had a problem, and one-third believed health care staff knew what they were doing.
In response, UConn Health launched an automated scheduling system to track the time between inmate requests for care and completion of services.
The plan was to repeat the survey the following year to see if there had been improvement, Sandra Tanguay, the operation administrator of CMHC, wrote at the time. After all, an annual survey was – and remains – a requirement in the contract between the correction department and UConn Health.
But it never happened.
The state’s auditors noticed the lack of follow-through, and concluded in an audit released last spring that the correction department, “did not provide evidence of oversight of the contractual terms.”
“Many elements of the [contract] have not been reviewed by DOC, resulting in DOC operating under the assumption of compliance by [UConn] with no corroborating evidence or attestation,” auditors John Geragosian and Robert Kane wrote of their review of operations for 2012 and 2013.
Perhaps most noticeable: None of Connecticut’s adult prisons currently are accredited by either the American Correctional Association or the National Commission on Correctional Health Care (NCCHC) – certifications that help validate quality.
The contract requires NCCHC accreditation.
The York Correctional Institution in East Lyme – Connecticut’s lone women’s prison – was the only prison accredited by NCCHC, but that ended this year.
Gail Johnson, interim executive director of prison health care at UConn Health, said becoming accredited is a huge effort “because of the paper nature of our environment.” Because UConn does not have an electronic health records system for its inmate services, Johnson said, becoming accredited requires going through individual patient files.
And so a decision was made not to accredit prisons “because of budget constraints with the fees involved and with manual tracking,” said Johnson. But, she added, staff in the state’s prisons and halfway houses are expected to follow the accreditation standards and are trained based on them.
“As the budget was cut back, something had to go. Were they going to cut nurses or were they going to not be reviewed?” Shelton asked. “They don’t have the time or money to deal with these systems issues.”
James Pavletich, leader of the NCCHC, said accreditation demonstrates that the care being provided is following best practices, and his organization helps systems improve if they fall short.
“Any correctional health care system that is struggling with quality should work toward accreditation,” he said.
Scott Semple, Connecticut’s correction commissioner since 2015, said he has not ruled out getting prisons NCCHC accredited.
“That’s not off the table. It may be one of the things that we want to strive for,” he said during an interview.
“Currently, we have not supported [ACA] accreditation of any of our facilities, but we do follow the accreditation standards. So in essence, we are doing the standards, but we are not paying for it.”
In addition, the prison infirmaries are not licensed by the Connecticut Department of Public Health, which oversees health care facilities throughout the state. The hospitals where inmates are sent for services not available at the prisons are licensed, however.
Staffing costs are the the main obstacle to accreditation rather than the fees, officials say. Connecticut has two jails for youths accused of crimes, both operated by the Judicial Branch rather than DOC. Both facilities have NCCHC accreditation; and the annual fee is $2,640. The annual fee for accreditation of a large adult prison in other states can be up to $15,000.

The state’s jail for youths convicted of offenses not serious enough to land them in the adult system – the Connecticut Juvenile Training School, which is run by the Department of Children and Families – has ACA accreditation, a $15,000 fee every three years.
Research limited
One expert says the state also has resisted another form of outside evaluation: academic research.
Shelton, the former UConn nursing professor who also is director of the Center for Correctional Health Research Networks, said it’s “very difficult” to do academic research in prisons.
“They do not want eyes in. They would prefer not,” she said of Connecticut.
Many inherent obstacles exist when doing research with a heavily controlled population, Shelton said, such as having a group-therapy space that prison staff can monitor for safety but where they aren’t close enough to overhear. Computer and reading restrictions and correction staff worries about researchers’ safety are also challenges.
“You are considered a safety hazard,” said Shelton. “Even if the DOC is agreeable, you have to get the buy-in from the facility too. You can get it done, but it is a very long and time-consuming process.”
Complaints aplenty
The Connecticut Office of the Attorney General over the last 10 years has logged more than 1,000 complaints and lawsuits from inmates about the health care they did or didn’t receive, or about inadequate accommodations for their medical conditions.
But it is hard to draw conclusions about whether these indicate systemic problems because the state does not track in any searchable way the resolution of the complaints and lawsuits. It also makes it incredibly time consuming to determine if there has been an uptick in allegations.
Allegations currently facing the state include a lawsuit from 48-year-old James Harnage, who is serving a 40-year sentence for multiple sexual offenses. He alleges medications are not being properly provided for pain in his feet, bowel distress, allergies and several other ailments. Another is from 38-year-old Wayne World, who is serving a 17-year sentence for manslaughter. He alleges staff delayed identifying and properly treating his skin cancer, despite his rapidly deteriorating condition.
In the case of the young woman giving birth in her cell on Feb. 13 – a case that has drawn complaints from various civil rights groups – staff were aware that she was pregnant, but the leaders of the correction department and UConn’s inmate health have differing versions of what happened.
Semple, the correction commissioner, told state legislators that his preliminary investigation shows, “The correctional staff did their job and that they were trying to communicate with the nurses that were assigned and were not getting an appropriate response.”
While UConn’s hospital in Farmington has a wing for scheduled procedures for inmates, emergencies are handled at the closest hospital to a prison. The inmate who gave birth in her cell was supposed to go to Lawrence and Memorial Hospital in New London.
But Johnson, the head of inmate care for UConn Health, said the birth happened early in the morning and was extremely quick so there was not enough time to get the inmate to the hospital.
“Sometimes this happens. She was a month premature. No one was expecting this to happen that quickly,” she said. “We did have nurses in there who have labor and delivery experience. They knew how to treat her, how to take care of the baby. They did what they would have done in a community hospital…It was actually a very good outcome, even though it may not have happened traditionally. You know if she would have gone to the hospital, she would have been chained to the bed; here she was in a cell. So you know, sometimes the perception sounds terrible but the reality is that she was very grateful for the help she was given for delivering her child.”
An official with the correction department said, however, its policies forbid using such restraints when a woman is in labor.
“… It’s unfortunate that we just hear about the one birth that happens in the cell, but how many births every week, month and year where that doesn’t happen?” she said.
So do the complaints and situations like the prison birth indicate systemic problems?
“Let me answer it this way: I don’t know of a health care delivery system that exists that hasn’t experienced some bad outcomes,” said Semple, the correction commissioner. “I think what people might tend to take for granted is that we have had numerous positive outcomes, but I am not going to say that we haven’t had circumstances that we were not in agreement on with UConn Health.”
The state has twice contracted with outside experts to assess inmate health care during Semple’s tenure. Requests made beginning Feb. 1 by The Connecticut Mirror to the correction department and the governor’s office for any documentation of those assessments have gone unfulfilled.
One of the reports, Semple said, is an expert’s findings on “some specific cases that were brought to my attention about concerns about the quality of health care for a very small group of people.” Because the report may reveal the department’s legal strategy in future litigation, the report’s entire contents are exempt from public disclosure, he said.
“I felt I needed to have some reliance on some outside set of eyes,” Semple said of the $63,000 contract with the Criminal Justice Institute, Inc.
The second consultant is A Health Adventure, Inc, whose work cost the state about $600,000. In announcing the department’s decision to begin managing inmate health care itself, a press release stated the decision was “principally based” on that consultant’s recommendations.
Since then, the department has been unable to say when or if those recommendations will be available. A correction official on Feb. 21 said the department has 21 information requests to fulfill before considering The Mirror’s Feb. 1 request for its release. Requests by The Mirror to the governor’s office for help overcoming the backlog of information requests were unsuccessful.
State vulnerable to criticism
The absence of outside oversight makes the state vulnerable to criticism.
“There is no constituency looking out for, and empowered to look out for, these inmates in Connecticut. Inmates have to go on bended knee begging for care,” said Dan Barrett, legal director for the American Civil Liberties Union of Connecticut.
His organization believes that inmates receiving poor care aren’t outliers, and that there is a larger problem.
“The birth in the cell, that’s just the tip of the iceberg. The conditions in prison are absolutely medieval,” said Barrett. “Connecticut is typical in that its system permits a ton of discretion of what services are provided. They are free to delay or ignore.”
While his office regularly gets complaints from inmates, his small staff of attorneys is only able to do so much.
Other watchdogs have struggled as well – or have closed.
A prison ombudsman’s office – opened in the early 1980s after a riot at a prison in Somers – closed in 2009. The annual $300,000 cost paid for a staff to investigate complaints and work with the correction department to resolve them.
“The law was repealed under the fiscal crisis,” said James R. Bookwalter, who served as ombudsman for decades.
The office’s closure left inmates having to log complaints with the department or file lawsuits. State funding for legal services for inmates has been cut too, however.
The state Auditors of Public Accounts – whose office is responsible for reviewing all state agencies’ performance – has 19 fewer auditors than in 2011, a 16 percent decline, because of the state’s fiscal problems. And so the most recent audit of correctional health care covers operations five years ago.
Disability Rights Connecticut – formerly Connecticut’s Office of Protection and Advocacy for Persons with Disabilities – not long ago had two advocates who did a lot of work in the state’s prisons. Then the state drastically scaled back its aid.
“We don’t have any advocates that are able to go out to the prisons at this point,” said Nancy Alisberg, the nonprofit’s legal director.
Now, when letters come from inmates requesting help getting mental health services, “It’s a question of whether we have the resources to help … We are much smaller now, but we still get the letters.”
Alisberg, an attorney behind a successful lawsuit in the late 1980s that changed how prisoners with mental illness must be treated, was unsure whether services have deteriorated.
The state’s child advocate, whose budget also has been cut, has the ability to investigate care being provided to youths confined in the state’s adult prisons as well as those cared for by all other state agencies that deal with children.
Two years ago, the child advocate concluded that the youths convicted of offenses too serious to go into the juvenile justice system were not receiving adequate mental health care at the correction department’s prison for young offenders.
“Youth at [Manson Youth Institute] did not receive rehabilitative or mental health treatment services commensurate with their needs,” the child advocate reported.
Only three of the 74 confined youths were determined by prison staff to need regular work with clinical professionals, though 71 of the youths had a history of struggling with mental health.
A self-monitoring system
Connecticut doesn’t currently compare well to other states in measuring the quality of medical and mental health care provided to inmates, according to a survey released last fall by The Pew Charitable Trusts and the Vera Institute of Justice.
“Connecticut is one of the states that doesn’t have what we consider a quality measurement system,” said Maria Schiff, a senior officer at Pew, a nonprofit national think tank.
Thirty-five states met the criteria, which included the use of data vs. anecdotes, identification of high-performing facilities, and somewhat regular measurement of performance. While having electronic health records makes it easier to monitor quality, most prisons in California and Massachusetts don’t have electronic records and still have quality measurement systems that meet Pew’s standards.
When an inmate dies while incarcerated, Connecticut is one of just four states that does not formally require a peer review – in which a broad array of staff review the case to determine whether the death could have been prevented.
“They do investigate deaths on an informal basis,” Pew reported.
UConn Health officials say they have set high standards and regularly spot-check cases.
“We do have a quality program. We do some performance measures. They are probably not as robust as we would like to see them because we don’t have an electronic health record … so we monitor by a sample of charts,” said Johnson.
The quality of those reviews is expected to improve in April when the correction department plans to launch an electronic health records system for inmates, she said.
“It should be much easier to monitor quality,” Johnson said.
Shelton said it also will improve care by providing better access to an inmate’s medical history.
State has cut funding
UConn’s Health’s inmate health program wasn’t shielded from the state budget axe wielded to close deficits. Over the last decade the state has pared funding by $26.8 million, a one-quarter reduction.
And in the fiscal year that begins July 1, another $8 million is scheduled to be cut. (These figures do not include state spending on employee health and retirement benefits, costs largely outside UConn’s control. Last fiscal year they totaled $53.7 million.)
Research by Pew shows Connecticut spending on inmate health remained steady at about $5,500 per-inmate between 2007 and 2015. While that puts Connecticut in the middle-of-the-pack among states, Pew’s Schiff said it is hard to know what to make of the figure as it relates to quality because of rising treatment costs and what the needs of inmates may be, which may be offset some by a declining prison population. Connecticut also has the lowest rate in the country of inmates older than 55, a group that typically cost much more to provide care.
“The question is what is Connecticut getting for the spending,” Schiff said.
UConn officials say the cuts are the reason the university wants to shed its responsibility for inmate health.
“It wasn’t because of quality,” Dr. Andrew Agwunobi, the chief executive officer of UConn Health, said during an interview. “We came to the Department of Correction and we said to them, ‘At the level of cuts we are seeing in this contract – initially we were losing $1 million and that was about two years ago … So we collaboratively started meeting with the department and started discussing what’s the solution.”
“We can’t make an $8 million cut and provide the same services. It’s just too much money, and there are costs that are increasing all the time,” said UConn’s Johnson.

Semple agreed with how the split happened. “They wanted to move in a different direction,” he said.
To make up for cuts in the past, UConn reduced staffing for inmate care and cut pharmaceutical and medical supply budgets. But Agwunobi said the spending cuts “were not related to a reduction in need.”
William Garrity, a nurse at UConn Health and president of the union that represents pharmacists, technicians and other staff, said workers, “share many of the concerns raised in the state auditors’ report – especially those related to patient care.”
“Cost issues are also not insignificant,” he said. “Years of disinvestment at UConn Health have taken a toll.”
These budget pressures are not unique to Connecticut.
“In any correctional system, it’s a really contentious system trying to balance a budget and trying to get the best care,” said Shelton, the editor of the inmate health academic journal. “The ratios of professional staff to inmates is way greater than you would find in any hospital.”
While UConn Health is a huge enterprise – with medical and dental schools, a hospital, outpatient clinics and research labs – those operations are unable to compensate for the state cuts for inmate health care. The health center has been fiscally ill for years, but the financial picture is the worst it has been in a long time, Agwunobi told his governing board last spring when it approved his $1.1 billion budget.
The correction department says it’s still fleshing out what its health care delivery system will look like. But Semple said he imagines it will be some sort of hybrid, including Department of Correction employees (many of whom he hopes to retain from UConn Health) and outside vendors.
But management responsibilities will fall on him, and eventually on whomever the next governor chooses as commissioner next year.
“When the day is done, I’m going to have to own this. So I would rather have some more ability to have control of what the administrative function of that would look like,” said Semple.
But the goal is to save the $8 million the adopted state budget calls for next year.
“We don’t anticipate that the budget reductions will reduce or diminish the quality of health care,” which Semple said is now is adequate. “The new health care delivery system is expected to operate more efficiently and provide community-standards level of care at a reduced budget.”
Union leader Garrity said switching management won’t solve the underlying problems.
“The issues identified by the auditors and the events in the past year demand greater oversight, but those promoting this latest proposal should demonstrate it actually accomplishes that objective,” he said. “As caregivers, we have an obligation to sound the ‘patient bed alarm’ when safety is at risk.”
Shelton, who has researched various prison health care delivery models, isn’t convinced either.
“Around and around and around we go,” she said, predicting a tumultuous transition. “You are not really solving the systems issues [by changing management] … Whether care will improve remains to be seen; I am not holding out birthday candles on that one. I think when you make a massive change, it takes years for things to settle.”
Updated on March 9 to reflect that the correction department’s policies do not permit restraining women during labor.


