



MIDDLETOWN – Ken knows there were many signs of how bad things got when he was drinking. Like the people who told him they were worried – the woman at the bank he’d done business with back when he was a successful mortgage broker, the office manager at his doctor’s office, the friend who kicked him out of his home, saying he didn’t want to watch Ken kill himself.
There was the year he spent in prison after his third time getting caught driving drunk.
Then there were the emergency room visits. Sometimes he went because his Crohn’s disease flared up, but often it was because of the drinking, and the depression it would provoke.
“When you start knowing people on a first-name basis in the ER, the nurses and the doctors, something’s wrong,” said Ken, 39, who spoke to The Mirror on the condition that his last name not be used.
Ken’s frequent trips to the Middlesex Hospital ER hardly made him unique. Like most hospitals, it had a stream of “super users” — patients who cycle in and out of the emergency room, using a large amount of health care resources that often have little impact on the psychiatric or social service needs that keep them coming back.
“Many of these people fall between the cracks of many service provision systems, but the one place where they keep emerging is in the emergency room,” said Lydia Brewster, assistant director for community services at St. Vincent de Paul Middletown, which operates a supportive housing program and a soup kitchen. “The emergency room knows they’re not solving the problem. They’re getting the person band-aided together.”
There are broader implications for the health care system too. Nationwide, 5 percent of patients accounted for half of total health care spending in 2012, according to federal data. Some health experts view focusing on “super users” as a key strategy in the quest to improve care while controlling health care costs.
But doing so requires grappling with a host of issues the medical system hasn’t traditionally been set up to handle: How do you identify and address the problems that keep people coming back to the ER, which are often related to homelessness, addiction, mental illness, and social service needs? How do you help patients navigate a fragmented care system that can be challenging for even the most informed to figure out?
In Ken’s case, one solution was relatively simple: He needed to go to detox. But he wasn’t ready to agree to it. On one of his many ER visits, a doctor ordered him to go, using a legal mechanism that allows a physician to commit a patient. Ken called his mother — a retired nurse — to ask if that was legal.
“Kenny, they can legally do that if they feel you’re a liability to yourself or you’re going to hurt yourself or somebody,” she said.
He called a lawyer friend. Same answer.
So he went for 72 hours. He told them what he thought they wanted to hear and quit drinking for two weeks.
Six months later he was back in the ER, in crisis.
Tracking the super users

What does it take to change things for patients like Ken?
Those are the sorts of questions that bring people from more than a dozen agencies to a windowless Middlesex Hospital conference room every Tuesday afternoon. Laptops open, they spend an hour brainstorming how to better meet the needs of Middletown-area super users.
The Community Care Team, as it’s known, tracks 208 patients — including Ken — and tries to coordinate their care, aiming to get at the underlying issues that keep them coming back to the ER, sometimes 80 times in a year. Participation is voluntary; clients sign a release allowing team members to share information about them with others on the team, which includes people working in emergency medicine, mental health, social services, care coordination and housing. It also includes Brewster, from the soup kitchen.
Terri DiPietro, Middlesex Hospital’s director of outpatient behavioral health, presents the cases. At a recent meeting, she noted that one client had been to the ER 15 times in the past two weeks. “Some days he comes in twice,” she said.
(The Community Care Team allowed a reporter to attend a recent meeting, during which members did not refer to clients by name or use identifying details.)
The cases brought up a variety of issues: Domestic violence. A history of sexual abuse. Anxiety. Addiction.
There were clients who wanted to go to detox but couldn’t get in – or wouldn’t stay in.
DiPietro was worried a client wasn’t taking her medications, so one team member — Elisabeth Spratto, who works for Community Health Network of Connecticut, which administers the medical portion of the state’s Medicaid program — offered to look the woman up in the system to see if she had picked up her prescriptions.
Later, when discussing another client, Spratto and Shevonne Mack, her counterpart from ValueOptions, which administers the behavioral health side of Medicaid, determined that the client had made 20 visits to four different emergency rooms in recent months. And, Mack reported after consulting her laptop, the client was now in another hospital.

That alone can be informative: Often, providers don’t realize how often their clients come to the ER, DiPietro said.
Some discussions turned to the problems hampering clients’ ability to stay sober or take care of their health. After a lengthy discussion of one client’s struggles, one clinician summed it up: “She’s lonely.”
Others centered on what service would be most appropriate for a client — physical therapy? Occupational therapy? A medical device? And which provider should offer it?
Having a range of providers in one room can make it easier to find services — an alternative to calling around, Brewster said.
“Instead of having it take weeks of trying to get through to the right person at the right agency, to say, ‘I think Joe needs substance abuse treatment, can we get him a bed?’…We can at this one meeting every week just sort of fly through the list of people, and in a very creative way, come up with care plans that sometimes involve the services of many of our agencies,” she said.
Forty percent of the team’s clients have been or are homeless or at the edge of homelessness. Forty percent have both a serious mental illness and addiction; another 54 percent have either a chronic mental illness or chronic alcoholism. Many also have complex medical problems.
The results have been encouraging team members say: Among those in the program for at least six months, ER and inpatient visits dropped by 1,142 compared to the same time period before the program, saving an estimated $1.7 million, according to the team’s data. One patient alone had 106 fewer visits; others saw 98- and 90-visit reductions, although not everyone had such pronounced drops in hospital visits – or any decrease.
It has taken relatively little money; there’s only one staffer paid by the program. But the effort relies on things that are less tangible – commitment, cooperation and time from people in many organizations.
Other hospitals in Connecticut have also started community care teams, and the two-year state budget legislators adopted last month includes $4.5 million over two years for grants for similar programs.
“We were spending a lot of money to help people die, in my mind, or to get worse,” DiPietro said. “Whereas now we’re focusing less of that money on helping people to get into recovery and sustain that.”
In the ER, a changing view
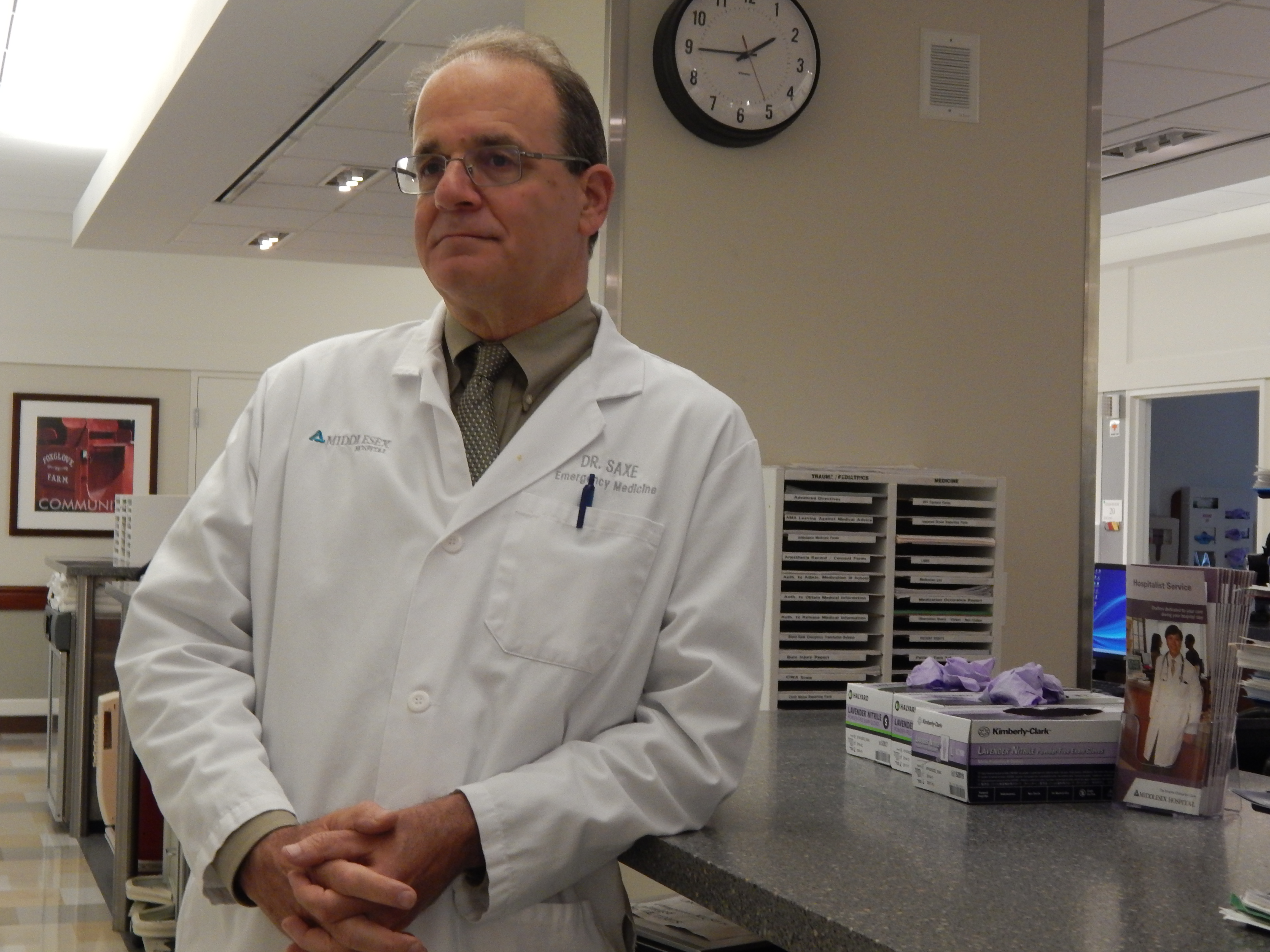
Next to DiPietro at the meeting sat Dr. Michael Saxe, the hospital’s chairman of emergency medicine. Until a few years ago, he saw the ER’s role as clear-cut: taking care of those who came through the doors. It didn’t involve anything that went on in the community.
But increasingly, patients with mental health needs or addictions were filling ER beds, staying longer than other patients, sometimes requiring someone to watch them if there was a risk of harm. They’d cycle in and out, and stretch the department’s ability to care for other patients.
And Saxe came to believe his department should get involved in ensuring those patients’ needs could be addressed in the community.
The team’s interventions come big and small. Often, the team works to try to find clients housing, which can bring a level of stability, as well as more concrete things, like a place to store medication.
When a client gets into stable housing, ER visits drop by an average of 80 percent, Saxe said.
“If you don’t know where you’re sleeping tonight, or what you’re going to eat, people can’t think about anything else. They’re not going to go to a follow-up doctor if they don’t have those things met,” said Margaret O’Hagan-Lynch, director of the addiction services division at Connecticut Valley Hospital, the state psychiatric hospital in Middletown.
“You’re just trying to survive the day,” Saxe said.
Sometimes the key interventions are small things that DiPietro summed up as “human kindness.”
“I think when you’re in a vulnerable place yourself, it can kind of give you the lift that you need, of, ‘Well, they cared enough…then maybe I need to care about myself a little bit more too,’” DiPietro said. “And I know that sounds overly simplistic, but we’ve seen it happen here before.”
‘Like having your own personal counselor’

For insights, the team often turns to Ijoma Okwuosa – known as IJ, the team’s one paid staffer. His title is health promotion advocate, but the most important part of his job might be that he loves to listen to people – and he’s not one of the clinicians looking to interview them for the next treatment decisions. He finds clients often want to talk.
“What’s really key is finding out what it is that drives them to the [ER],” he said.
Okwuosa’s phone rings a lot. Doctors call if they suspect a patient fits the criteria for the community care team – five ER visits in six months. Clients call to talk or if they’re having a problem. Sometimes he tries to find them a bed in a facility to avoid their having to stop in the ER. He’s always trying to solve a problem: Where should this patient go? Can I help them now? Tomorrow?
Often, Okwuosa is the one who tells a potential client about the team and asks them to sign a release to participate. Only two have said no, and both were actively psychotic, DiPietro said. They later agreed.
Okwuosa was Ken’s link to the team. They met during one of Ken’s trips to the hospital’s crisis unit – the secure unit for people in psychiatric crisis. He and Okwuosa hit it off.
“It’s almost like having your own personal counselor,” Ken said.
When they met, Ken wasn’t ready to get help.
For years, he’d been a functioning alcoholic. He earned six figures as a mortgage broker. He was out and social, partying. Then things started to spiral down. The housing crash hurt his business. His father died. His mother, who he considered his backbone, went to a nursing home. “It kind of killed me inside, more than I thought,” Ken said.
Starting in 2010, he went on what he calls a three-year tear – at one point, drinking two pints of 100-proof vodka a day. And he went into a depression. He felt hopeless, and, at some points, suicidal.
“I knew in the back of my mind if I didn’t do something soon or come to terms or something, I would be dead,” he said.
On one of his ER visits, Okwuosa told Ken, “You really need to get some help. You got a good life ahead of you still.”
“And that didn’t stick,” Ken said.
Trying again
Those on the team say it’s common for the first plan not to work. They frequently revise and tweak the care plans.
But they say they can see results.
The amount of time patients with behavioral health problems spend in the emergency room – which is typically far longer than medical patients – has dropped by nearly 35 percent at Middlesex, from 24 to 16 hours, Saxe said.
It’s demoralizing for emergency room staff to care for the same patient, with the same problems, visit after visit, Saxe said. Having the team in place has given them some hope, he said.
Each client has an ER care plan in case they come to the emergency room. It might be to refrain from prescribing narcotics if the client has a history of addiction. Or to notify DiPietro or Saxe immediately so they can work with community agencies to address the person’s needs. There might be a plan to have a patient committed to detox.
If a patient says he’s working with a certain community provider, the ER staff will call the provider.
“Before that never would’ve happened,” said Barbara Durham, senior lead case manager for Advanced Behavioral Health, a team member. “And it ties all this together, so that we’re treating the whole person.”
One thing the Community Care Team is not: a quick fix. The work will continue indefinitely, Saxe said. “It’s not something you can fix and then walk away from.”
‘Something clicked’

The last time Ken was in the crisis unit, Okwuosa asked him, why don’t you go to detox?
He didn’t want to.
But a week later, “Something clicked with me,” he said. “Maybe God helped me.”
He called Merritt Hall, the addiction treatment facility at Connecticut Valley Hospital, and said he wanted to come in. He did – after a detour to do 14 shots.
When he arrived, they asked how he was. “I don’t know, but I’m here so let’s get to work,” he said he told them. “And I knew right there and then, I knew from that day on that my life would be different.”
Not that it was easy.
“It was very tough for me to really come to terms with it,” Ken said.
And then there was what came next.
“What scared me about inpatient rehab was getting out,” he said. “All the safety net’s gone.”
The team had arranged for Ken to have a spot in a dual-diagnosis program after he got out. One thing they’ve learned, DiPietro said, is that as soon as a client enters a facility, they need to start planning the next step, for when they get out and are particularly vulnerable to relapse.
Ken has been sober for more than a year. He says his life has come together. He now has a peace of mind he didn’t have while drinking.
“I knew I was very depressed when I drank alcohol,” he said. “I didn’t realize how deeply I was into it until I got out of it for a few months.”
He got his drivers’ license back. He wants to help others going through what he did. He says he’s lucky; his friends stuck by him.
“I talk to a lot of bar owners now that I see, and they [say], ‘Dude, we’re so glad you stopped drinking,’” he said.
He still has the DUIs on his record, something that will turn up on background checks when he applies for jobs. He still thinks about alcohol three or four times a week. But he remembers what it brought him.
“The more time that goes on, it gets a little easier,” Ken said. “But you still can’t forget where you were at.”
A few months ago, stomach problems landed him back in the ER. He worried the doctors would think he was back for drinking again.
The nurse greeted him: “How ya doing, Ken?”
“I’m not here for drinking!” he assured her.
The staff said they understood.
“You don’t want to be labeled as that,” Ken said. “It’s a tough thing to overcome, and you want to show people that you’re moving on.”