


In the 1990s, then-Senator Joe Biden and others pushed a War on Drugs, a war that had a tremendous negative impact on our state. Prison populations soared; over a third of young men of color were under criminal justice supervision; and drug use and attendant public health consequences proceeded unabated.
State and local budgets were skewed toward punishment rather than public health treatment of drug dependence and related diseases such as AIDs, tuberculosis, and hepatitis. Recognizing those impacts, in 1997 the Judiciary Committee of the Connecticut General Assembly asked the Connecticut Law Revision Commission to review the state’s policies toward illegal drugs. The Commission recommended 23 changes in Connecticut law to reduce the state’s emphasis on a criminal justice and to focus instead on a public health response to illegal drugs.
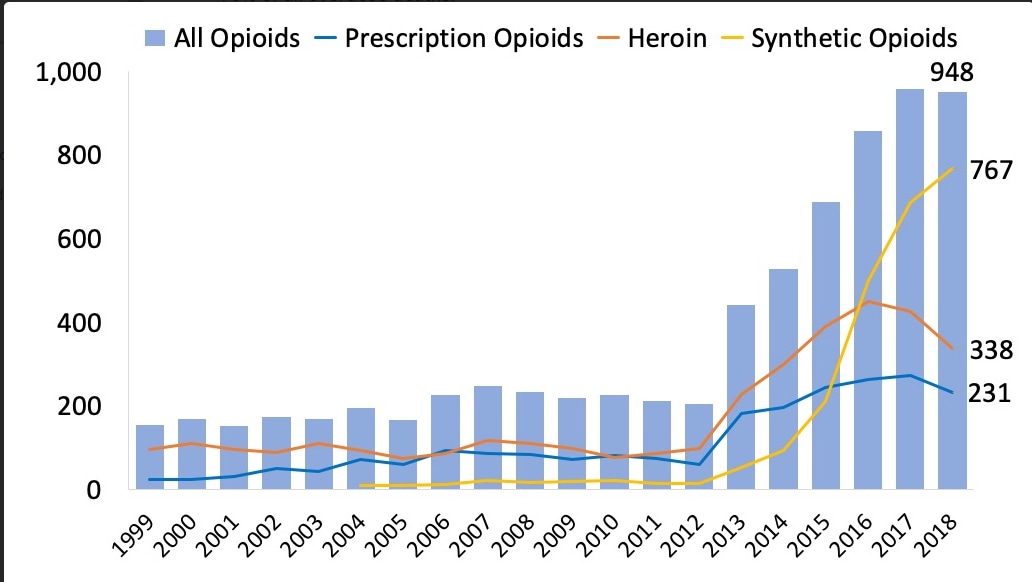
Sadly, some of the more significant recommendations were not implemented. The fallout of that failure is now apparent. Recent news reports point to the state’s expanding crisis in opioid overdoses and deaths that continue to bedevil Connecticut and its public health and criminal justice systems.
Now, the Biden administration’s American Rescue Plan recognizes that a public health approach is critical to addressing substance dependence. Billions of new federal dollars have been committed to that effort. Connecticut needs to take robust advantage of those federal dollars. Unlike some public investments, the individual and state economic benefit of a new effort will become apparent almost immediately through reduced strains on public health and criminal justice resources. Below are ways the state can refocus to a public health approach.
- Use medication to reduce opioid overdose deaths: Naloxone is the single most effective medication to reduce opioid overdose deaths. CT simply does not have enough commitment to and access to naloxone.
- Screen each prisoner for OUD (opioid use dependence) immediately on intake at state prisons and jails– both for pretrial inmates and on sentencing.
- Link immediate screening with immediate — not delayed — treatment, including methadone and similar medications. There is no medical reason to delay methadone treatment at intake.
Although methadone treatment has been used for decades at York women’s prison, the Department of Corrections (DOC) has vigorously opposed the treatment for male prisoners. The department has now begun limited testing of methadone treatment for male prisoners. For best results, however, screening and methadone treatment ought now be universal, not merely a test and should begin on admission to incarceration.
- Link intake screening with HIV/HCV testing.
- Link each methadone patient on release with placement in a community methadone program.
- Detoxify prisoners with OUD with buprenorphine. DOC medical officials do not use buprenorphine broadly or adequately enough to detoxify prisoners with OUD.
- Require methadone treatment to be available in all out-of-jail criminal justice diversionary programs. Each criminal justice diversionary program, not some, should have methadone treatment available for each individual with OUD in the program. These programs include CT half-way houses, work release programs, transitional programs, alternative sanctions programs, re-entry and post-release programs, etc. Too often, some programs use only abstinence treatment – a treatment that does not use medications and that does not have the record of success that medication treatment has.
- Increase state fiscal support for medication (methadone and buprenorphine) OUD treatment and make support sufficient to meet the need.
- State support is so low that engaging a sufficient number of medication treatment providers is difficult.
- State-supported transportation to medication treatment programs can be problematic because of unreliable transportation vendors or delay in distributing bus passes. Thus, patients don’t get to appointments and treatment providers don’t get paid for non-appearing patients.
- Review whether it is appropriate, both fiscally and for better public health, to continue the limited state funding for abstinence treatment programs – programs that do not provide methadone or buprenorphine for OUD or detoxification. Only medication-based treatment programs have a solid record of success treating OUD.
- Change the law to allow 24-hour access to naloxone and sterile needles at medication dispensing units.
- Support telehealth advice for behavior health. After the Covid emergency, continue reimbursement for telehealth for behavioral health.
- Create safe injection rooms. Establish a pilot program to determine whether supervised, safe injection rooms improve health and social functioning outcomes. Other states and countries have such programs. Yale had expressed some interest in piloting such a program.
- Allow private physicians to dispense methadone to patients after being stabilized at a methadone clinic.
- Review drug sentencing laws. Review whether the length of sentences for drug-related offenses is still appropriate. Many of these sentences were established decades ago during the War on Drugs and many might be the result of implicit racial bias.
- Engage with the Yale School of Public Health working group on Covid and substance treatment for further recommendations.
Connecticut now has an opportunity to move beyond a War on Drugs ideology and toward the most effective treatments available for OUD, reduce opioid overdose deaths, and reduce attendant societal costs.
David D. Biklen of West Hartford was Executive Director of the Connecticut Law Revision Commission when it issued its drug policy recommendations.