



Prison doctors made a series of requests in October 2017 for patients to see specialists. One inmate had diabetes and was losing sensation in his feet. Another needed special shoes because all of his toes had been amputated due to frostbite. A third patient’s prosthetic foot was worn out with tears and holes and needed to be repaired.
It appears they were all denied care. But the state can’t say for sure.
That’s because officials from the state Department of Correction and the University of Connecticut Health Center, which until recently managed the $100 million-plus inmate health care system, didn’t keep records of the panel that made these final decisions.

With no record-keeping system – which was required under UConn Health’s contract with the state – it is impossible to determine if appropriate health care was delivered to the 13,000 inmates in state prisons on any given day.
That leaves lawmakers and civil rights groups – who have growing concerns about the quality of health care provided to inmates – with no way to gauge whether recent disturbing stories shared by inmates and their families, as well as numerous lawsuits against the state, are proof of a systemic failure or simply isolated incidents in an otherwise functioning process.
While UConn Health was responsible for the management of the Utilization Review Committee, which vetted requests from prison doctors, the Department of Correction’s contract with the university required the state be given quarterly utilization reports detailing “The number of requests, percentage of denials, reasons for denial (categories), approvals and missed appointment ratios.”
The utilization committee, which had the final say over whether treatment would be provided, didn’t keep minutes of their meetings or decisions. State records retention policies require state agencies to retain health utilization records for five years.
UConn’s internal policy also required they maintain a “utilization review log” and a “ticker tracking system” regarding requested care for inmates – and the outcomes.
It didn’t happen.
“There’s no tracking system that I was able to find,” said Scott Simpson, an attorney for UConn Health, when asked during an interview why the university would not be able to provide the records.
Simpson said the most recent leader of inmate health care at UConn Health told him the university never kept such records. This is one of several quality-assurance measures the agency’s contract required, but were not followed.
The CT Mirror requested records regarding the outcomes of doctors’ requests from UConn Health on Nov. 16 under the state’s Freedom of Information law. It took officials there nearly a month to disclose they never collected the data.
The importance of a tracking system became apparent during the legislative hearing last July. That hearing capped months of concerns from lawmakers and civil rights groups about the quality of medical and mental health care being provided to inmates.
A month later, the state paid a former inmate $1.3 million after he claimed staff delayed identifying and properly treating his skin cancer for more than a year, despite his rapidly deteriorating condition.
Amid these mounting concerns about the lack of oversight for inmate health care – and with UConn Health officials signaling drastic state funding cuts had taken their toll – DOC Commissioner Scott Semple decided the agency would assume management of inmate care starting July 1.
The legislature allocates funding for inmate health care as a block grant, rather than as payment for services provided. As a result, UConn Health received a lump sum every year, which meant services were constrained by the size of the grant.
Semple, who is retiring at the end of the year after 30 years with DOC, said during an interview with the public affairs radio show Where We Live earlier this month that ending the relationship “was a two-way street.”
“When you are dealing with different entities and trying to navigate through improving health care, it’s easier when it falls under the agency so we can have more direct control,” he said.
A handwritten ‘Yes’ or ‘No’?
When initially asked for the data, UConn officials directed the CT Mirror to the DOC for records, saying they lost access to the electronic system when the correction department assumed management of inmate health.
Officials at DOC quickly refuted they have the data.
Karen Martucci, who handles information requests for the DOC, said, “Bottom line, I am unable to provide data related to the approval or denial rates from their committee. I don’t have access to that information.”
UConn Health later acknowledged the data was probably never collected, but officials there were eventually able to provide a small window into how requests were handled by the committee.
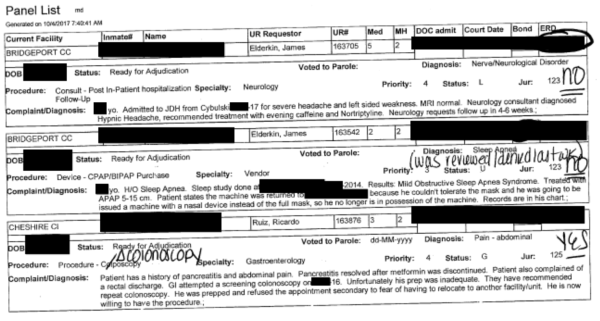
The agency released redacted copies of “panel lists” — or doctors’ requests — from the month of October 2017. Some of the entries on those lists contain handwritten notes of “yes” or “no,” presumably indicating whether the request was approved or denied.
UConn Health officials warned against drawing any conclusions about whether the “yes” or “no” markings that adorn the doctor’s requests to the panel meant the individual was approved to receive care, but believe that’s what the notes meant.
Of the 707 doctors’ requests made during October 2017, 79 had a “no” written next to the request, 448 had a “yes,” and the remaining 180 did not contain any indication of the resolution.
Two of the “no” indicators were for the podiatry services referenced at the beginning of this story. The third had no stated outcome.
That was the request made on behalf of the amputee whose prosthetic foot was worn out. The person who reviewed this request did not give a definitive yes or no, simply writing, “It was fine for him in community, this will be costly!”
Inmate stories: outliers or the norm?
Purplish black flare-ups and open sores marked inmate Wayne World’s body, but a prison doctor’s request for a dermatology consult was denied by the utilization committee.
The biopsy that was eventually ordered was delayed for months, and when it finally was performed several months later, the results were inconclusive. It would take several more months before Wayne received another biopsy.

In response to World’s grievance about the nearly two-year delay, the reviewer responded that “the doctors who consult on UR cases make recommendations, not orders” and that those decisions are for the Utilization panel to make.
Complaints from World’s mother eventually led to the correction department’s health director to order her nurse to do a special review of the case.
He took issue with the care provided.
“My concerns [were] that the care wasn’t timely enough,” Nurse Timothy Bombard, testified in relation to the lawsuit that led to the $1.3 million settlement.
World was one of seven medical cases the DOC settled with inmates since July 2017 without admitting fault. Those other settlements ranged from $300 to $15,000.
| Inmate | Settlement | Date opened | Allegation |
|---|---|---|---|
| Wayne World | $1,300,000 | 4/1/16 | Delayed diagnosis and treatment for cancer |
| Samuel See | $15,000 | 12/24/16 | Medical staff ignored history of phyciatric issues, died in detention |
| Shawn Milner | $13,500 | 12/22/16 | Denied access to seizure medication |
| Luis Torres | $8,000 | 7/27/17 | Delayed medical care after being assaulted |
| Christopher Brown | $5,000 | 12/25/16 | Assaulted by a correction officer |
| Franklin Gelinas | $500 | 4/1/17 | Not disclosed |
| Anthony Cannon | $300 | 7/2/15 | In a car accident when being transported to court, denied MRI |
There are at least six other current lawsuits related to inmate heath care, while a number of additional cases are headed toward legal action.
One of those inmates was misdiagnosed with a sinus infection for about nine months when he really had stage 4 nasopharyngeal cancer—leaving him with a tumor the size of a baseball in his sinus cavity. Another, who died last year, was misdiagnosed with reflux disease when he actually had stage 4 cancer in his larynx.

Bombard – who was part of a team of 11 medical providers employed by the DOC to oversee the health care UConn provided to inmates – estimated specialized care requested by prison doctors was denied by UConn’s panel 20 to 30 percent of the time.
Dr. Joseph Breton, who was appointed in March as DOC’s chief medical officer and resigned three months later, testified in World’s case the panel regularly interfered with providing care patients needed.
Breton, who became a prison physician in 2015 after working in a private practice as a primary care doctor for more than a decade, said he got “a multitude of denials in a row.”
“I believe the delay in care was harmful,” he said. “I come from a different world, right, so if I need something fixed, I can fix it quickly… I obviously began to see that there was a marked difference between community and inside.”
Health care staff who work in the prisons said during recent interviews that treatment was routinely denied or delayed.
“Oh, God. They were waiting months – months – for an outside appointment, if it happened at all,” said Kelly Schabot, a social worker at Carl Robinson Correctional Institution in Enfield.
“Outside appointments were always something they had to wait for, and then costs were a huge factor in determining whether services would be available,” said Lydia Rostkowski, a nurse supervisor at McDougall Walker Correctional Institution in Suffield, who has worked in various state prisons for 10 years. “No one would say, ‘Well, it costs this much [so] it’s not approved.’ But a request was sent to the committee and then it would not be approved.”
But UConn has never tracked this information, according to officials there.
“UConn does not maintain any aggregate data reports regarding the number of UR Committee requests, approvals and costs,” said Megan Philippi, who handles Freedom of Information requests for UConn. “To the best of our knowledge, UConn never maintained such records.”
Dan Barrett, the legal director of the state’s chapter of the ACLU, takes issue with the lack of oversight.
“At best, it looks incompetent. It looks as though DOC failed to look at and supervise its contractor to see if health care was being provided,” he said. “And at worst, it confirms the suspicion of those who think the URC was used to deny medical care to prisoners.”
Fast forward: a yes for every request
When the state correction department took over managing inmate health care five months ago, the commissioner promised he would be able to save millions.
This promise was made in the wake of state appropriations for inmate health care being cut 24 percent over the last 10 years – going from $107 million to $81 million since 2008.
This year, another $9 million was cut. Five months into the fiscal year, inmate health care is expected to cost the department $15 million more this year than budgeted.
Helping drive that deficit is the DOC’s decision to approve every request prison doctors make for specialized care or treatment.
Now solely managing the inmate health care system, the DOC was able to readily provide documentation of how requests are being handled. Data provided to the CT Mirror show the state has approved every request made for treatment since the transition from UConn Health.
That meant in October 2018 that each of the 742 requests were approved compared to 448 of the 707 requests that UConn Health officials believed were approved in October 2017.
“There is clearly a lot of trust that is being placed in the physicians,” said Martucci, the spokeswoman for the DOC.
Front-line staff have noticed the change.
“Now if a doctor decides they need something … they just get it. That has been an improvement. The appointments are getting scheduled now and inmates are getting that higher level of care that they need,” said Rostkowski, the nurse supervisor.
It won’t be this way for much longer, as the department is in the process of setting up a system it’s dubbed “PPT” that will determine “community standards of care” to determine what level of care will be provided. This is akin to private health care paying for certain services, and not others, Martucci said.
When asked why required oversight was never provided, Martucci said the department is looking forward, not back.
“The Department of Correction is placing the focus on the future state of our healthcare delivery system. Although it will take some time to measure success, we believe we are moving in the right direction with a process, the PPT, that enhances access to care,” she said.
Treatment, if there’s a doctor to see
Inmates still can face long waits for a referral since appointments with a prison doctor or nurse are often delayed. That’s because DOC had not hired any new front-line staff in the five months since the transition until Dec. 7, when seven new employees began work.
Ninety positions remain vacant – roughly 15 percent of all medical staff.
“Multiple prisons don’t have a doctor,” said Schabot, the social worker.
“Without the front-line staff to bring them in for sick call – and when there is no doctor to see them – that impedes the process to move forward and get care,” said Robert Ramonas, a nurse supervisor at Garner Correctional Institution in Newtown.
“Hiring the staff we need would mean that an inmate could see a doctor in days rather than waiting for months,” said David Pickus, president of SEIU 1199, the union that represents many of the medical staff. “This decision to underfund services has serious consequences for human lives.”
Schabot, a social worker, said, “We can only do so much in a shift. We can only help so many people. This is not why we went into this profession … We’ve been very quiet for a lot of years [about] how the budget cuts have impacted the prisons.”
The department was unable to provide details on how long inmates have been waiting to see a physician, but agreed staffing is an issue.
“We’ve done some hires, but we’re not nearly where we need to be or have to be,” Martucci said. “The process is long, it’s complicated. It’s the state’s process.”
She reports at least 25 medical staff positions are in the final stages of the hiring process and are expected to be filled in January.
All of this is enough to convince some that inmates are not getting proper health care.
State Senate Republican leader Len Fasano, who previously appealed for a public hearing and “full transparency” to assess allegations of poor health care in state prisons, said he is very concerned about inmate health care.

“When you have a no-bid contract, these are the types of things that happen … no matter what the outcome is, frankly no one cares about the outcome,” Fasano said. “I would consider their management to be below the standards that are required for quality care.”
Attorney Kenneth Krayeske, who represented World with Attorney DeVaughn Ward, said “there were breakdowns in every possible place you could have system failures” and there is no oversight over what happens at the most basic level of inmate care.
The attorney said he believes the lack of adequate care stems from understaffing and the stigma of being a prisoner.
“So there becomes a cultural chilling effect that the URC panel created by saying ‘OK, if you do this enough times you’re going to understand what’s going to get accepted and what’s going to get rejected, so you’re just going to stop asking for medical care for these patients because you know it’s not going to happen, so why waste your time?’” Krayeske said.